Department of Radiology, Mayo Clinic, Rochester, MN, USA.
Department of Neurological Sciences, Rush University, Chicago, IL, USA.
Alzheimers Dement. 2018 Apr;14(4):535-562. doi: 10.1016/j.jalz.2018.02.018.
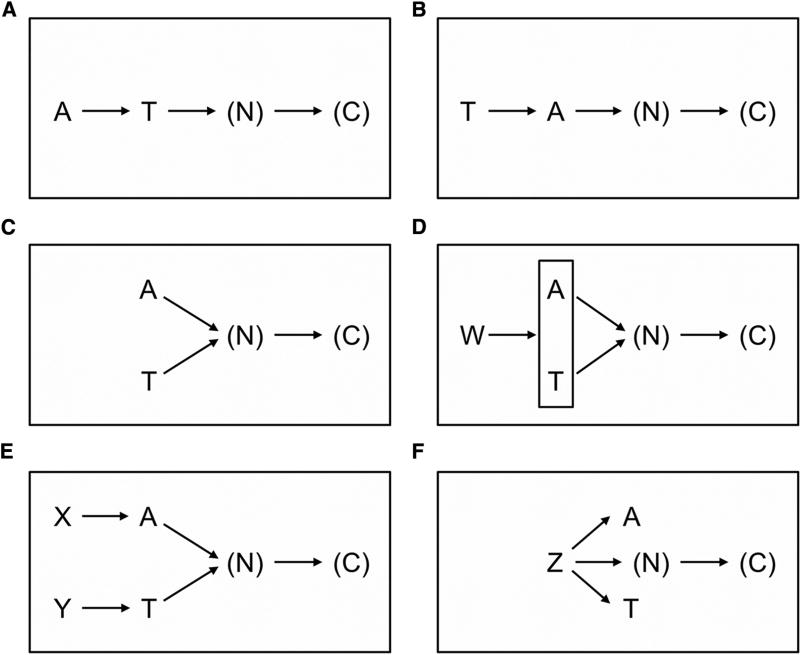
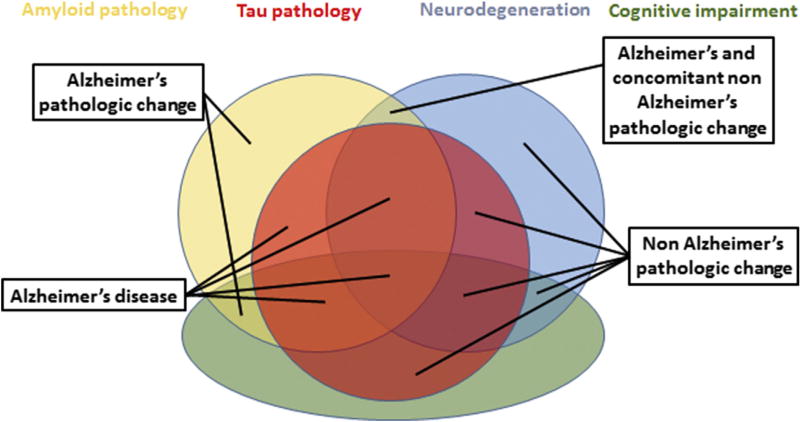
In 2011, the National Institute on Aging and Alzheimer's Association created separate diagnostic recommendations for the preclinical, mild cognitive impairment, and dementia stages of Alzheimer's disease. Scientific progress in the interim led to an initiative by the National Institute on Aging and Alzheimer's Association to update and unify the 2011 guidelines. This unifying update is labeled a "research framework" because its intended use is for observational and interventional research, not routine clinical care. In the National Institute on Aging and Alzheimer's Association Research Framework, Alzheimer's disease (AD) is defined by its underlying pathologic processes that can be documented by postmortem examination or in vivo by biomarkers. The diagnosis is not based on the clinical consequences of the disease (i.e., symptoms/signs) in this research framework, which shifts the definition of AD in living people from a syndromal to a biological construct. The research framework focuses on the diagnosis of AD with biomarkers in living persons. Biomarkers are grouped into those of β amyloid deposition, pathologic tau, and neurodegeneration [AT(N)]. This ATN classification system groups different biomarkers (imaging and biofluids) by the pathologic process each measures. The AT(N) system is flexible in that new biomarkers can be added to the three existing AT(N) groups, and new biomarker groups beyond AT(N) can be added when they become available. We focus on AD as a continuum, and cognitive staging may be accomplished using continuous measures. However, we also outline two different categorical cognitive schemes for staging the severity of cognitive impairment: a scheme using three traditional syndromal categories and a six-stage numeric scheme. It is important to stress that this framework seeks to create a common language with which investigators can generate and test hypotheses about the interactions among different pathologic processes (denoted by biomarkers) and cognitive symptoms. We appreciate the concern that this biomarker-based research framework has the potential to be misused. Therefore, we emphasize, first, it is premature and inappropriate to use this research framework in general medical practice. Second, this research framework should not be used to restrict alternative approaches to hypothesis testing that do not use biomarkers. There will be situations where biomarkers are not available or requiring them would be counterproductive to the specific research goals (discussed in more detail later in the document). Thus, biomarker-based research should not be considered a template for all research into age-related cognitive impairment and dementia; rather, it should be applied when it is fit for the purpose of the specific research goals of a study. Importantly, this framework should be examined in diverse populations. Although it is possible that β-amyloid plaques and neurofibrillary tau deposits are not causal in AD pathogenesis, it is these abnormal protein deposits that define AD as a unique neurodegenerative disease among different disorders that can lead to dementia. We envision that defining AD as a biological construct will enable a more accurate characterization and understanding of the sequence of events that lead to cognitive impairment that is associated with AD, as well as the multifactorial etiology of dementia. This approach also will enable a more precise approach to interventional trials where specific pathways can be targeted in the disease process and in the appropriate people.
2011 年,美国国家老龄化研究所和阿尔茨海默病协会(Alzheimer's Association)为阿尔茨海默病的临床前期、轻度认知障碍和痴呆阶段分别制定了单独的诊断建议。在此期间,美国国家老龄化研究所和阿尔茨海默病协会提出了一项倡议,旨在更新和统一 2011 年的指南。这一统一更新被标记为“研究框架”,因为其预期用途是用于观察性和干预性研究,而不是常规临床护理。在该研究框架中,阿尔茨海默病(AD)是由其潜在的病理过程定义的,可以通过尸检或体内生物标志物来证实。该诊断不是基于该疾病的临床后果(即症状/体征),因此,在该研究框架中,活人的 AD 定义从综合征转变为生物结构。该研究框架专注于使用生物标志物对活人体内的 AD 进行诊断。生物标志物分为β淀粉样蛋白沉积、病理性 tau 和神经退行性变 [AT(N)]。该 ATN 分类系统根据每种测量方法所测量的病理过程对不同的生物标志物(成像和生物液)进行分组。该 ATN 系统具有灵活性,可将新的生物标志物添加到现有的三个 AT(N)组中,并且当出现新的 AT(N)以外的生物标志物时,也可以将其添加到该系统中。我们关注 AD 作为一个连续体,认知分期可以使用连续测量来完成。然而,我们还概述了两种用于分期认知障碍严重程度的不同分类认知方案:一种方案使用三个传统的综合征类别,另一种方案使用六级数字方案。重要的是要强调,该框架旨在用一种通用语言来生成和测试关于不同病理过程(由生物标志物表示)和认知症状之间相互作用的假设。我们理解人们担心这种基于生物标志物的研究框架有可能被滥用。因此,我们首先强调,在一般医疗实践中,目前使用该研究框架还为时过早,也不合适。其次,该研究框架不应用于限制不使用生物标志物的替代假设检验方法。在某些情况下,生物标志物不可用,或者要求使用生物标志物可能会对特定的研究目标产生反作用(在本文档的后面更详细地讨论)。因此,基于生物标志物的研究不应被视为与年龄相关的认知障碍和痴呆研究的所有研究的模板;而是应该在该研究特定目标的具体研究目的下应用。重要的是,该框架应在不同人群中进行检验。尽管β-淀粉样斑块和神经纤维缠结 tau 沉积可能不是 AD 发病机制中的因果关系,但正是这些异常蛋白沉积将 AD 定义为不同可导致痴呆的神经退行性疾病中的一种独特疾病。我们设想,将 AD 定义为生物结构将使我们能够更准确地描述和理解导致与 AD 相关的认知障碍的一系列事件,以及痴呆的多因素病因。这种方法还将使我们能够更精确地进行干预试验,从而可以针对疾病过程中的特定途径以及适当的人群进行靶向治疗。