Balan Daniel, Martha Orsolya, Chibelean Calin Bogdan, Tataru Sabin, Voidezan Septimiu, Sin Anca, Matei Victor Deliu, Vartolomei Mihai Dorin, Lucarelli Giuseppe, Cioffi Antonio, Del Giudice Francesco, De Berardinis Ettore, Borda Angela, Busetto Gian Maria, Ferro Matteo, Pytel Akos, Porav-Hodade Daniel
Department of Cell and Molecular Biology Department of Urology, University of Medicine and Pharmacy, Tirgu Mures, Romania Department of Urology, University of Pécs, Pécs, Hungary Department of Epidemiology, University of Medicine and Pharmacy, Tirgu Mures, Romania Division of Urology, European Institute of Oncology, Milan, Italy Department of Urology, Medical University of Vienna, Vienna, Austria Department of Emergency and Organ Transplantation-Urology, Andrology and Kidney Transplantation Unit, University of Bari, Bari Department of Urology, Sapienza University of Rome, Rome, Italy Department of Histology, University of Medicine and Pharmacy, Tirgu Mures, Romania.
Medicine (Baltimore). 2018 Apr;97(16):e0522. doi: 10.1097/MD.0000000000010522.
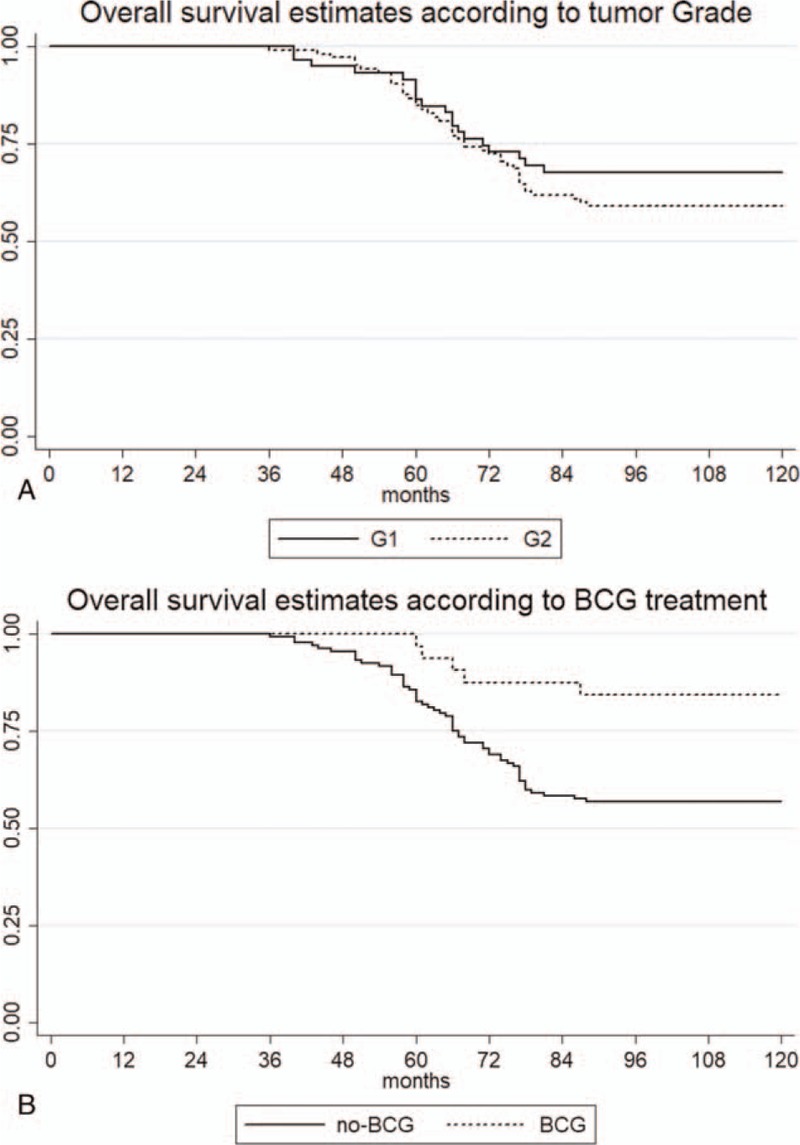
To compare long-term overall survival (OS) in patients with G1 and G2 grade Ta bladder cancer after transurethral resection of bladder tumors (TURBTs). Secondary aim was to investigate clinical and pathologic prognostic factors for OS of Ta patients, except G3/high grade (HG).A total of 243 patients, retrospectively selected, with Ta nonmuscle invasive bladder cancer (NMIBC) underwent TURBT between January 2006 and December 2008 (median follow-up 109 months). Inclusion criteria were: Ta at first manifestation, G1 or G2 grade with no associated carcinoma in situ (CIS). Seventy-nine patients were excluded due to concomitant CIS (1), G3/HG tumors (47), and lost to follow-up (31). Ethical approval was obtained from the Ethical Committee of the Mures County Hospital. Statistical analysis was performed using STATA 11.0.Following inclusion criteria, 164 patients with primary G1 or G2 Ta tumors, were enrolled. Recurrence was observed in 26 (15.8%) and progression in 5 (3%) patients. Ten-year survival in G1 patients was 67.8% (CI 54.3-78.1) and in G2 patients 59% (CI 49-67.3) (P = .31). Univariable and multivariable logistic regression analysis underlined that advanced age at diagnosis (hazard ratio [HR] 1.10) and no Bacillus Calmette-Guerin (BCG) treatment (HR 0.24 and 0.29) were independent predictors for death at 10 years after diagnosis.Long-term analysis confirms that patients with well differentiated (G1) and moderately well differentiated (G2) Ta tumors have similar OS. A longer OS was even reported in those who underwent BCG adjuvant therapy.
比较经尿道膀胱肿瘤切除术(TURBTs)后G1和G2级Ta期膀胱癌患者的长期总生存率(OS)。次要目的是研究除G3/高级别(HG)外Ta期患者OS的临床和病理预后因素。
回顾性选取2006年1月至2008年12月期间共243例接受TURBT的Ta期非肌层浸润性膀胱癌(NMIBC)患者(中位随访109个月)。纳入标准为:首次表现为Ta期,G1或G2级且无原位癌(CIS)。79例患者因合并CIS(1例)、G3/HG肿瘤(47例)和失访(31例)被排除。获得了穆列什县医院伦理委员会的伦理批准。使用STATA 11.0进行统计分析。
按照纳入标准,纳入了164例原发性G1或G2 Ta期肿瘤患者。26例(15.8%)患者出现复发,5例(3%)患者出现进展。G1级患者的10年生存率为67.8%(CI 54.3 - 78.1),G级患者为59%(CI 49 - 67.3)(P = 0.31)。单变量和多变量逻辑回归分析强调,诊断时年龄较大(风险比[HR] 1.10)和未接受卡介苗(BCG)治疗(HR 0.24和0.29)是诊断后10年死亡的独立预测因素。
长期分析证实,高分化(G1)和中分化(G2)Ta期肿瘤患者的OS相似。接受BCG辅助治疗的患者甚至报告有更长的OS。