Cardoso João, Coelho Ricardo, Rocha Carla, Coelho Constança, Semedo Luísa, Bugalho Almeida A
Department of Respiratory Medicine, Hospital de Santa Marta, Centro Hospitalar Lisboa Central, Lisboa, Portugal.
Nova Medical School/ Faculdade de Ciências Médicas, Universidade Nova de Lisboa, Portugal.
Int J Chron Obstruct Pulmon Dis. 2018 Apr 5;13:1105-1113. doi: 10.2147/COPD.S155848. eCollection 2018.
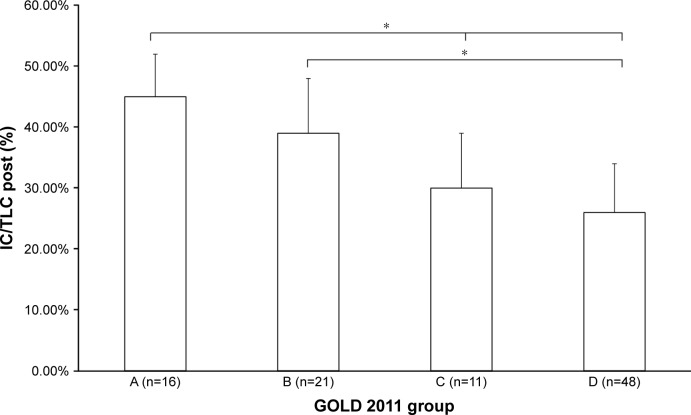
Severe exacerbations and mortality are major outcomes in COPD, and risk factors for these events are actively searched for. Several predictors of mortality have been identified in COPD. The inspiratory capacity/total lung capacity (IC/TLC) ratio has been shown to be a strong predictor of all cause and respiratory mortality in patients with COPD. The major objectives of this study were to analyze which clinical parameters, including lung volumes, were the best predictors of the 5-year cumulative risk of hospital admissions or death and the 5-year risk of exacerbations, in stable COPD patients.
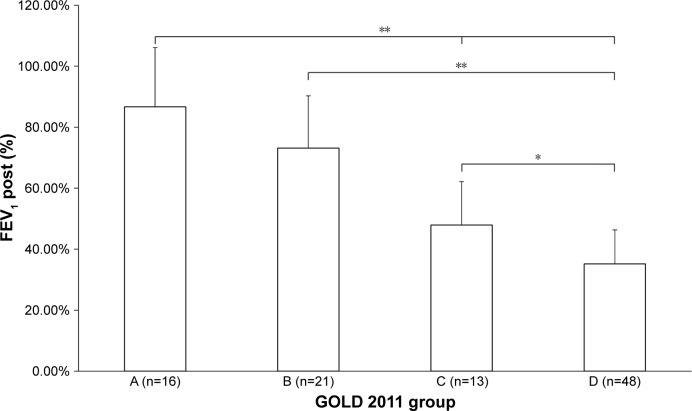
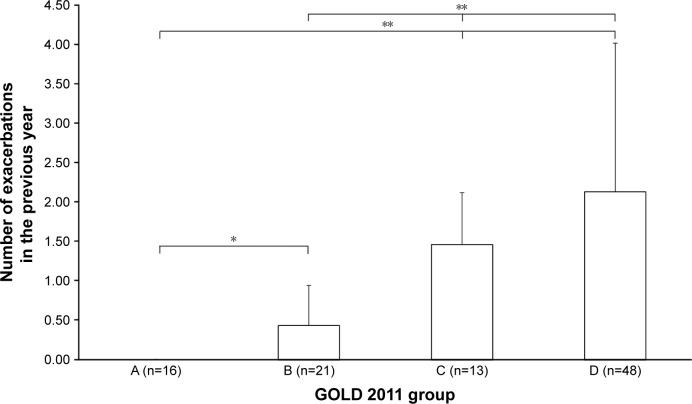
This study retrospectively reviewed data from 98 stable COPD patients, consecutively recruited in 2012. Forced expiratory volume in 1 s (FEV), modified Medical Research Council dyspnea scale, exacerbation history (ExH), Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2011 groups, and lung volumes were reviewed. Five years later, this population was evaluated for cumulative exacerbations, hospital admissions, and mortality. All the population, and GOLD group D separately, were analyzed.
The cumulative 5-year combined risk of hospital admission or death was significantly predicted by the ExH and the IC/TLC ratio. Analyzing separately group D, FEV was the only predictor of this outcome. The frequency of exacerbations in the previous year was the best predictor of future cumulative 5-year risk of subsequent exacerbations, both for the total population and the GOLD D group.
ExH and IC/TLC ratio were the best predictors of the most severe outcomes in COPD (admissions or mortality), independently of COPD severity. FEV was the only predictor of the cumulative 5-year combined risk of hospital admission or death in the GOLD D group. ExH was the best predictor of 5-year cumulative future risk of exacerbations. Besides FEV and ExH, the IC/TLC ratio can be a useful predictor of severe outcomes in COPD.
严重急性加重和死亡率是慢性阻塞性肺疾病(COPD)的主要结局,人们一直在积极寻找这些事件的危险因素。COPD中已确定了几种死亡率预测因素。吸气容量/肺总量(IC/TLC)比值已被证明是COPD患者全因死亡率和呼吸死亡率的有力预测因素。本研究的主要目的是分析哪些临床参数,包括肺容积,是稳定期COPD患者5年累计住院或死亡风险以及5年急性加重风险的最佳预测因素。
本研究回顾性分析了2012年连续招募的98例稳定期COPD患者的数据。回顾了第1秒用力呼气容积(FEV)、改良医学研究委员会呼吸困难量表、急性加重病史(ExH)、慢性阻塞性肺疾病全球倡议(GOLD)2011分组以及肺容积。5年后,对该人群进行了累积急性加重、住院和死亡率评估。对所有人群以及单独的GOLD D组进行了分析。
ExH和IC/TLC比值显著预测了5年累计住院或死亡的综合风险。单独分析D组时,FEV是该结局唯一的预测因素。前一年的急性加重频率是总体人群和GOLD D组未来5年后续急性加重累积风险的最佳预测因素。
ExH和IC/TLC比值是COPD最严重结局(住院或死亡)的最佳预测因素,与COPD严重程度无关。FEV是GOLD D组5年累计住院或死亡综合风险的唯一预测因素。ExH是5年未来急性加重累积风险的最佳预测因素。除了FEV和ExH外,IC/TLC比值可能是COPD严重结局有用的预测因素。