Rush University Medical Center, Chicago, IL.
Stanford University School of Medicine, Palo Alto, CA.
Hepatology. 2018 Oct;68(4):1298-1307. doi: 10.1002/hep.30046. Epub 2018 Jul 25.
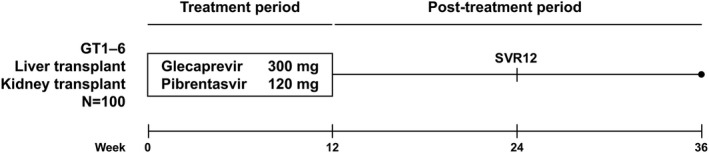
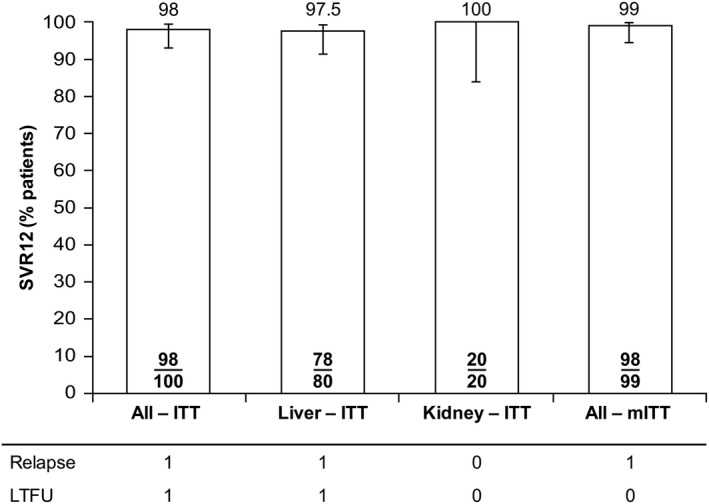
Well-tolerated, ribavirin-free, pangenotypic hepatitis C virus (HCV) treatments for transplant recipients remain a high priority. Once-daily glecaprevir/pibrentasvir demonstrates high rates of sustained virologic response at 12 weeks posttreatment (SVR12) across all major HCV genotypes (GTs). This trial evaluated the safety and efficacy of glecaprevir/pibrentasvir for patients with chronic HCV GT1-6 infection who had received a liver or kidney transplant. MAGELLAN-2 was a phase 3, open-label trial conducted in patients who were ≥3 months posttransplant. Patients without cirrhosis who were HCV treatment-naive (GT1-6) or treatment-experienced (GT1, 2, 4-6; with interferon-based therapy with or without sofosbuvir, or sofosbuvir plus ribavirin) received glecaprevir/pibrentasvir (300/120 mg) once daily for 12 weeks. The primary endpoint compared the percentage of patients receiving glecaprevir/pibrentasvir with SVR12 to a historic SVR12 rate based on the standard of care. Safety of glecaprevir/pibrentasvir was assessed. In total, 80 liver transplant and 20 kidney transplant patients participated in the trial. Most patients had no or minimal fibrosis (80% had fibrosis scores F0-F1) and were infected with HCV GT1 (57%) or GT3 (24%). The overall SVR12 was 98% (n/N = 98/100; 95% confidence interval, 95.3%-100%), which exceeded the prespecified historic standard-of-care SVR12 threshold of 94%. One patient experienced virologic failure. One patient discontinued because of an adverse event considered to be unrelated to treatment; this patient achieved SVR12. Adverse events were mostly mild in severity, and laboratory abnormalities were infrequent.
Once-daily glecaprevir/pibrentasvir for 12 weeks is a well-tolerated and efficacious, ribavirin-free treatment for patients with chronic HCV GT1-6 infection who have received a liver or kidney transplant. (ClinicalTrials.gov NCT02692703.) (Hepatology 2018; 00:000-000).
对于移植受者,耐受性良好且无利巴韦林的泛基因型丙型肝炎病毒(HCV)治疗仍然是当务之急。每日一次的格卡瑞韦/哌仑他韦在治疗后 12 周(SVR12)时,在所有主要的 HCV 基因型(GT)中均显示出高持续病毒学应答率(SVR12)。这项试验评估了格卡瑞韦/哌仑他韦用于慢性 HCV GT1-6 感染且已接受肝或肾移植患者的安全性和疗效。MAGELLAN-2 是一项 3 期、开放标签试验,在移植后≥3 个月的患者中进行。无肝硬化的初治(GT1-6)或经治(GT1、2、4-6;含干扰素为基础的治疗联合或不联合索磷布韦,或索磷布韦联合利巴韦林)的患者每日接受一次格卡瑞韦/哌仑他韦(300/120mg)治疗 12 周。主要终点是比较接受格卡瑞韦/哌仑他韦治疗的患者的 SVR12 比例与基于标准护理的历史 SVR12 率。评估了格卡瑞韦/哌仑他韦的安全性。共有 80 例肝移植和 20 例肾移植患者参与了这项试验。大多数患者无纤维化或仅有轻微纤维化(80%的纤维化评分 F0-F1),且感染 HCV GT1(57%)或 GT3(24%)。总的 SVR12 为 98%(n/N=98/100;95%置信区间,95.3%-100%),超过了预先指定的历史标准护理 SVR12 阈值 94%。1 例患者发生病毒学失败。1 例患者因被认为与治疗无关的不良事件而停药;该患者获得了 SVR12。不良事件大多为轻度,实验室异常少见。
每日一次的格卡瑞韦/哌仑他韦治疗 12 周,是一种耐受性良好且有效的、无利巴韦林的治疗方案,适用于已接受肝或肾移植的慢性 HCV GT1-6 感染患者。(ClinicalTrials.gov NCT02692703)。(《肝脏病学》2018 年;00:000-000)。