Division of Cardiovascular Medicine, University of Wisconsin School of Medicine and Public Health, Madison, WI.
Department of Cardiology, Arrhythmologic Centre, Ospedali del Tigullio, Lavagna, Italy.
J Am Heart Assoc. 2018 Apr 19;7(9):e008528. doi: 10.1161/JAHA.118.008528.
The mechanism of inappropriate sinus tachycardia (IST) remains incompletely understood.
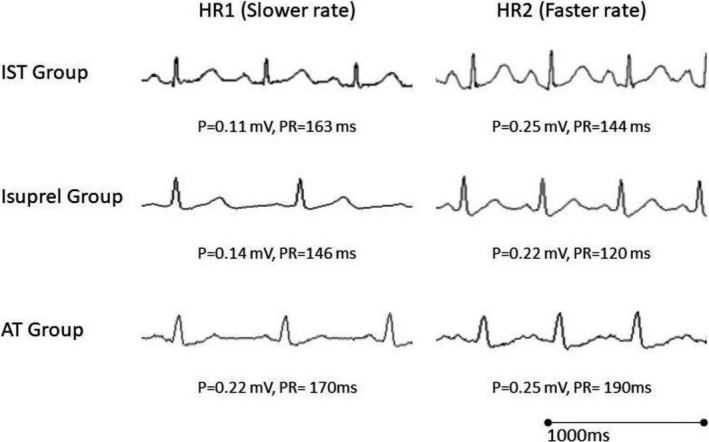
We prospectively compared 3 patient groups: 11 patients with IST (IST Group), 9 control patients administered isoproterenol (Isuprel Group), and 15 patients with cristae terminalis atrial tachycardia (AT Group). P-wave amplitude in lead II and PR interval were measured at a lower and higher heart rate (HR1 and HR2, respectively). P-wave amplitude increased significantly with the increase in HR in the IST Group (0.16±0.07 mV at HR1=97±12 beats per minute versus 0.21±0.08 mV at HR2=135±21 beats per minute, =0.001). The average increase in P-wave amplitude in the IST Group was similar to the Isuprel Group (=0.26). PR interval significantly shortened with the increases in HR in the IST Group (146±15 ms at HR1 versus 128±16 ms at HR2, <0.001). A similar decrease in the PR interval was noted in the Isuprel Group (=0.6). In contrast, patients in the atrial tachycardia Group experienced PR lengthening during atrial tachycardia when compared with baseline normal sinus rhythm (153±25 ms at HR1=78±17 beats per minute versus 179±29 ms at HR2=140±28 beats per minute, <0.01).
We have shown that HR increases in patients with IST were associated with an increase in P-wave amplitude in lead II and PR shortening similar to what is seen in healthy controls following isoproterenol infusion. The increase in P-wave amplitude and absence of PR lengthening in IST support an extrinsic mechanism consistent with a state of sympatho-excitation with cephalic shift in sinus node activation and enhanced atrioventricular nodal conduction.
不适当窦性心动过速(IST)的发生机制尚不完全清楚。
我们前瞻性比较了 3 组患者:11 例 IST 患者(IST 组)、9 例给予异丙肾上腺素(Isuprel 组)的对照患者和 15 例冠状窦终末嵴房性心动过速(AT 组)患者。在较低和较高心率(HR1 和 HR2)时测量 II 导联的 P 波振幅和 PR 间期。在 IST 组,P 波振幅随心率增加而显著增加(HR1=97±12 次/分时为 0.16±0.07 mV,HR2=135±21 次/分时为 0.21±0.08 mV,=0.001)。IST 组 P 波振幅的平均增加与 Isuprel 组相似(=0.26)。PR 间期随 IST 组心率的增加而显著缩短(HR1 时为 146±15 ms,HR2 时为 128±16 ms,<0.001)。Isuprel 组也观察到类似的 PR 间期缩短(=0.6)。相比之下,在 AT 组患者中,当房性心动过速时与基础窦性心律相比 PR 间期延长(HR1 时为 78±17 次/分,153±25 ms,HR2 时为 140±28 次/分,179±29 ms,<0.01)。
我们表明,IST 患者的心率增加与 II 导联 P 波振幅增加和 PR 缩短有关,与健康对照者异丙肾上腺素输注后所见相似。IST 中 P 波振幅增加和 PR 无延长支持一种外在机制,与窦房结激活的头部移位和房室结传导增强相一致的交感兴奋状态。