Ciani Oriana, Epstein David, Rothery Claire, Taylor Rod S, Sculpher Mark
1Evidence Synthesis and Modeling for Health Improvement, Institute of Health Research, University of Exeter Medical School, South Cloisters, St Luke's Campus, Exeter, EX1 2LU UK.
2Center for Research on Health and Social Care Management, SDA Bocconi University, via Roentgen 1, 20136 Milan, Italy.
Cost Eff Resour Alloc. 2018 Apr 16;16:15. doi: 10.1186/s12962-018-0098-7. eCollection 2018.
Fenestrated endovascular aneurysm repair (fEVAR) is a new approach for complex abdominal aortic aneurysms, limited to a few specialist centers, with limited evidence base. We developed a cost-effectiveness decision model of fEVAR compared to open surgical repair (OSR) to investigate the likely direction of costs and benefits and inform further research projects on this technology.
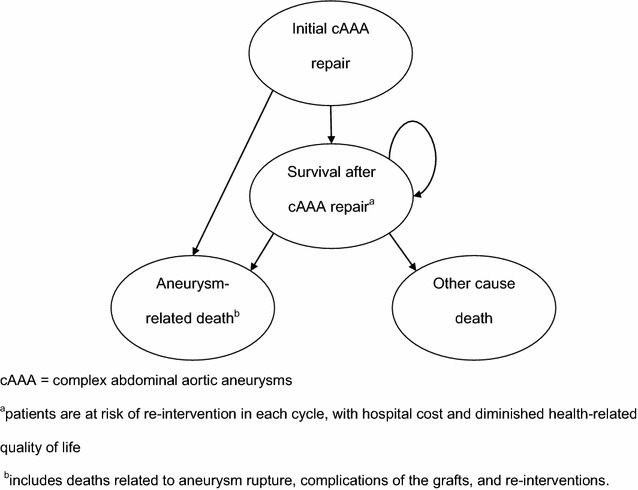
A systematic review with meta-analysis and a four-state Markov model were used to estimate the cost-effectiveness of fEVAR versus OSR. We used a recent coverage with evidence development framework to characterize the main sources of uncertainty and inform decisions about the type of further research that would be most worthwhile and feasible.
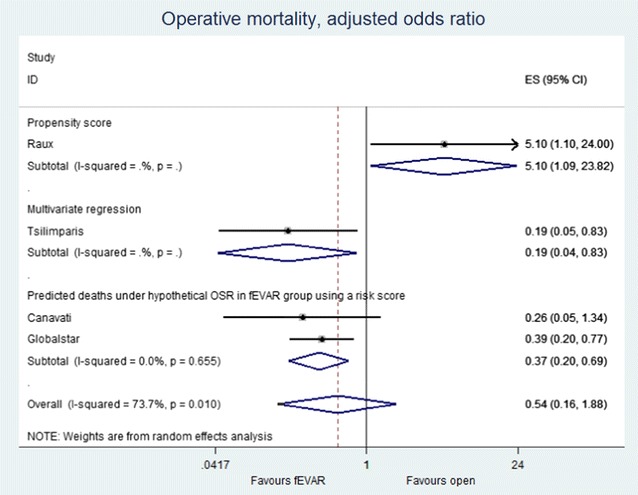
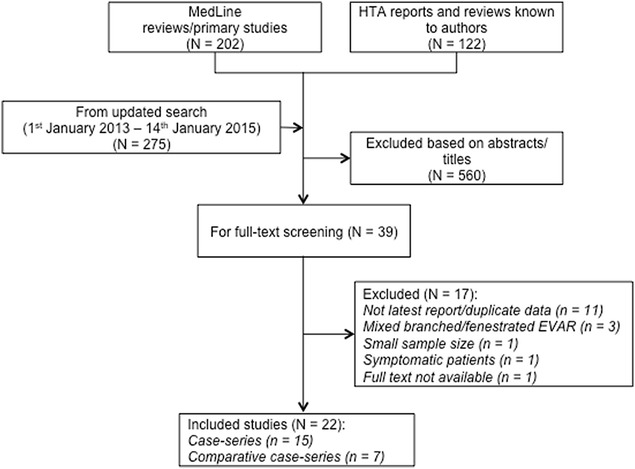
Seven observational comparative studies were identified, of which four presented odds ratios adjusted for confounders. The odds ratios for operative mortality varied widely between studies. Assuming a central estimate of the odds ratio of 0.54 (95% CI 0.05-6.24), the decision model estimated that the incremental cost per quality adjusted life year (QALY) was £74,580/QALY with a probability of 9 and 16% of being cost-effective at standard cost-effectiveness thresholds of £20,000/QALY and £30,000/QALY, respectively. The Expected Value of Perfect Information over 10 years at a threshold of £20,000/QALY was £11.2 million. Operative mortality contributed to most of the uncertainty in the decision model.
In the case of "maturing technologies", decision modelling indicates the likely direction of costs and benefits and guides the development of further research projects. In our analysis of fEVAR versus OSR, decision uncertainty, particularly around operative mortality, might be effectively resolved by a short-term RCT, or possibly a well-conducted comparative observational study. Decision makers may consider that a conditional coverage decision is warranted with assessments required to make this type of recommendation depending on local priorities and circumstances.
开窗型血管腔内动脉瘤修复术(fEVAR)是治疗复杂腹主动脉瘤的一种新方法,仅在少数专科中心开展,相关证据有限。我们建立了一个fEVAR与开放手术修复(OSR)对比的成本效益决策模型,以研究成本和效益的可能趋势,并为该技术的进一步研究项目提供参考。
采用系统评价及荟萃分析和四状态马尔可夫模型来估计fEVAR与OSR的成本效益。我们使用了一个近期的循证拓展覆盖框架来描述主要的不确定性来源,并为最有价值和可行的进一步研究类型的决策提供依据。
共纳入7项观察性对比研究,其中4项给出了经混杂因素调整的比值比。各研究之间手术死亡率的比值比差异很大。假设比值比的中心估计值为0.54(95%CI 0.05 - 6.24),决策模型估计每质量调整生命年(QALY)的增量成本为74,580英镑/QALY,在20,000英镑/QALY和30,000英镑/QALY的标准成本效益阈值下,具有成本效益的概率分别为9%和16%。在20,000英镑/QALY的阈值下,10年的完美信息期望值为1120万英镑。手术死亡率是决策模型中大部分不确定性的来源。
对于“成熟技术”,决策模型可表明成本和效益的可能趋势,并指导进一步研究项目的开展。在我们对fEVAR与OSR的分析中,决策不确定性,尤其是围绕手术死亡率的不确定性,可能通过短期随机对照试验或精心开展的对比观察性研究得到有效解决。决策者可能认为有必要做出有条件的覆盖决策,并根据当地的优先事项和情况进行评估以提出此类建议。