Division of Surgery and Interventional Science (SR), University College London, London, United Kingdom; Surgical and Interventional Trials Unit (RS, NW, CB-G), University College London, London, United Kingdom; Department of Urology, University College London Hospital (WST, PK, JDK), London, United Kingdom; University College London Cancer Institute (SR, AF), London, United Kingdom; Department of Urology, Royal Surrey County Hospital (HM), Guildford, United Kingdom; Department of Urology, James Cook University Hospital (JC), Middlesbrough, United Kingdom; Department of Urology, Western Sussex Hospitals NHS Foundation Trust, Worthing Hospital (JH), Worthing, United Kingdom; Department of Urology, East Surrey Hospital (AR), Redhill, United Kingdom; Department of Urology, Maidstone Hospital (AH), Maidstone, United Kingdom; Department of Urology, Pennine Acute Hospitals NHS Trust, North Manchester General Hospital (JC), Crumpsall, United Kingdom.
Division of Surgery and Interventional Science (SR), University College London, London, United Kingdom; Surgical and Interventional Trials Unit (RS, NW, CB-G), University College London, London, United Kingdom; Department of Urology, University College London Hospital (WST, PK, JDK), London, United Kingdom; University College London Cancer Institute (SR, AF), London, United Kingdom; Department of Urology, Royal Surrey County Hospital (HM), Guildford, United Kingdom; Department of Urology, James Cook University Hospital (JC), Middlesbrough, United Kingdom; Department of Urology, Western Sussex Hospitals NHS Foundation Trust, Worthing Hospital (JH), Worthing, United Kingdom; Department of Urology, East Surrey Hospital (AR), Redhill, United Kingdom; Department of Urology, Maidstone Hospital (AH), Maidstone, United Kingdom; Department of Urology, Pennine Acute Hospitals NHS Trust, North Manchester General Hospital (JC), Crumpsall, United Kingdom.
J Urol. 2018 Nov;200(5):973-980. doi: 10.1016/j.juro.2018.04.065. Epub 2018 Apr 24.
Computerized tomography urogram is recommended when investigating patients with hematuria. We determined the incidence of urinary tract cancer and compared the diagnostic accuracy of computerized tomography urogram to that of renal and bladder ultrasound for identifying urinary tract cancer.
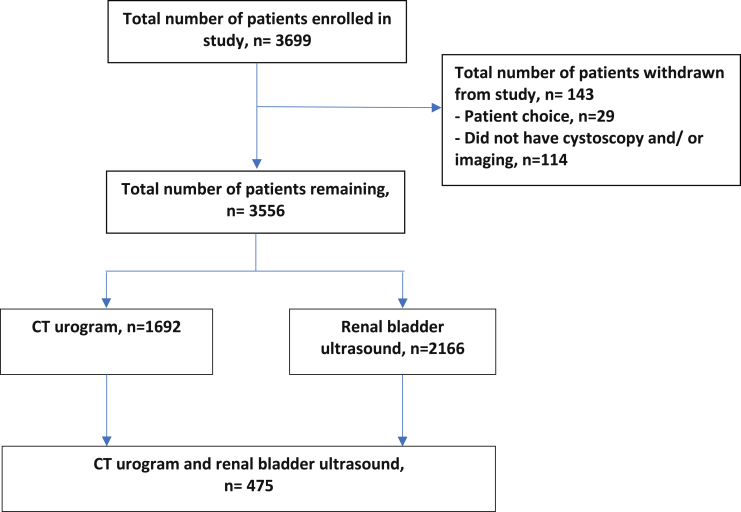
The DETECT (Detecting Bladder Cancer Using the UroMark Test) I study is a prospective observational study recruiting patients 18 years old or older following presentation with macroscopic or microscopic hematuria at a total of 40 hospitals. All patients underwent cystoscopy and upper tract imaging comprising computerized tomography urogram and/or renal and bladder ultrasound.
A total of 3,556 patients with a median age of 68 years were recruited in this study, of whom 2,166 underwent renal and bladder ultrasound, and 1,692 underwent computerized tomography urogram in addition to cystoscopy. The incidence of bladder, renal and upper tract urothelial cancer was 11.0%, 1.4% and 0.8%, respectively, in macroscopic hematuria cases. Patients with microscopic hematuria had a 2.7%, 0.4% and 0% incidence of bladder, renal and upper tract urothelial cancer, respectively. The sensitivity and negative predictive value of renal and bladder ultrasound to detect renal cancer were 85.7% and 99.9% but they were 14.3% and 99.7%, respectively, to detect upper tract urothelial cancer. Renal and bladder ultrasound was poor at identifying renal calculi. Renal and bladder ultrasound sensitivity was lower than that of computerized tomography urogram to detect bladder cancer (each less than 85%). Cystoscopy had 98.3% specificity and 83.9% positive predictive value.
Computerized tomography urogram can be safely replaced by renal and bladder ultrasound in patients who have microscopic hematuria. The incidence of upper tract urothelial cancer is 0.8% in patients with macroscopic hematuria and computerized tomography urogram is recommended. Patients with suspected renal calculi require noncontrast renal tract computerized tomography. Imaging cannot replace cystoscopy to diagnose bladder cancer.
当患者出现血尿时,建议进行计算机断层尿路造影检查。我们旨在确定尿路癌症的发病率,并比较计算机断层尿路造影与肾脏和膀胱超声检查对尿路癌症的诊断准确性。
DETECT(使用 UroMark 试验检测膀胱癌)I 研究是一项前瞻性观察性研究,在 40 家医院共招募了因肉眼血尿或镜下血尿就诊的 18 岁及以上患者。所有患者均接受了膀胱镜检查和上尿路影像学检查,包括计算机断层尿路造影和/或肾脏和膀胱超声检查。
本研究共纳入了 3556 例中位年龄为 68 岁的患者,其中 2166 例行肾脏和膀胱超声检查,1692 例除膀胱镜检查外还进行了计算机断层尿路造影检查。在肉眼血尿病例中,膀胱癌、肾癌和上尿路尿路上皮癌的发病率分别为 11.0%、1.4%和 0.8%。镜下血尿患者的膀胱癌、肾癌和上尿路尿路上皮癌的发病率分别为 2.7%、0.4%和 0%。肾脏和膀胱超声检查对肾癌的敏感性和阴性预测值分别为 85.7%和 99.9%,但对检测上尿路尿路上皮癌的敏感性和阴性预测值分别为 14.3%和 99.7%。肾脏和膀胱超声检查对肾脏结石的识别能力较差。肾脏和膀胱超声检查对膀胱癌的敏感性低于计算机断层尿路造影(均低于 85%)。膀胱镜检查的特异性为 98.3%,阳性预测值为 83.9%。
在患有镜下血尿的患者中,计算机断层尿路造影可安全地被肾脏和膀胱超声检查替代。在肉眼血尿患者中,上尿路尿路上皮癌的发病率为 0.8%,建议进行计算机断层尿路造影检查。疑似肾结石患者需要进行非增强性尿路计算机断层扫描。影像学检查不能替代膀胱镜检查来诊断膀胱癌。