Goodman David M, Srofenyoh Emmanuel K, Ramaswamy Rohit, Bryce Fiona, Floyd Liz, Olufolabi Adeyemi, Tetteh Cecilia, Owen Medge D
Department of Obstetrics and Gynecology, Hubert-Yeargan Center for Global Health, Duke University Medical Center, Durham, North Carolina, USA.
Department of Obstetrics and Gynecology, Greater Accra Regional Hospital, Ghana Health Service, Accra, Ghana.
BMJ Glob Health. 2018 Apr 17;3(2):e000623. doi: 10.1136/bmjgh-2017-000623. eCollection 2018.
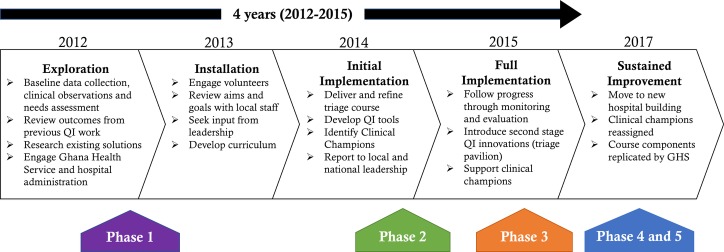
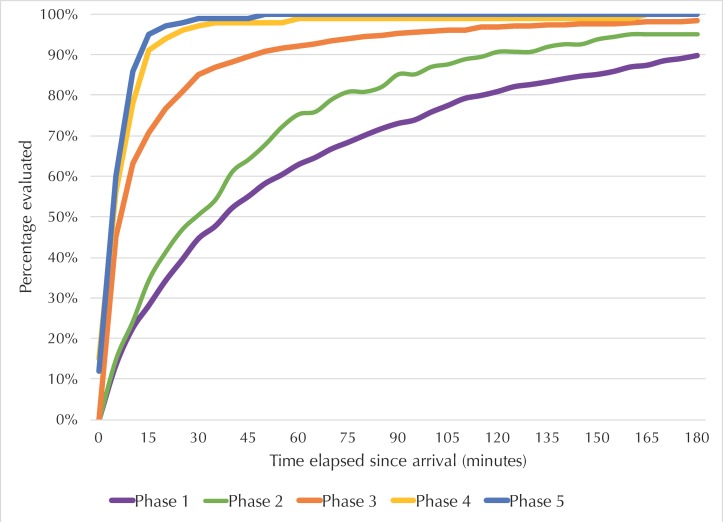
Institutional delivery has been proposed as a method for reducing maternal morbidity and mortality, but little is known about how referral hospitals in low-resource settings can best manage the expected influx of patients. In this study, we assess the impact of an obstetric triage improvement programme on reducing hospital-based delay in a referral hospital in Accra, Ghana. An Active Implementation Framework is used to describe a 5-year intervention to introduce and monitor obstetric triage capabilities. Baseline data, collected from September to November 2012, revealed significant delays in patient assessment on arrival. A triage training course and monitoring of quality improvement tools occurred in 2013 and 2014. Implementation barriers led to the construction of a free-standing obstetric triage pavilion, opened January 2015, with dedicated midwives. Data were collected at three time intervals following the triage pavilion opening and compared with baseline including: referral indications, patient and labour characteristics, waiting time from arrival to assessment and the documentation of a care plan. An obstetric triage improvement programme reduced the median (IQR) patient waiting time from facility arrival to first assessment by a midwife from 40 min (15-100) to 5 min (2-6) (p<0.001) over the 5-year intervention. The triage pavilion enhanced performance resulting in the elimination of previous delays associated with the time of admission and disease acuity. Care plan documentation increased from 51% to 96%. Obstetric triage, when properly implemented, reduced delay in a busy, low-resource hospital. The implementation process was sustained under local leadership during transition to a new hospital.
机构分娩已被提议作为降低孕产妇发病率和死亡率的一种方法,但对于资源匮乏地区的转诊医院如何最好地应对预期的患者涌入情况,人们了解甚少。在本研究中,我们评估了一项产科分诊改善计划对减少加纳阿克拉一家转诊医院基于医院的延误的影响。一个积极实施框架被用于描述一项为期5年的干预措施,以引入和监测产科分诊能力。2012年9月至11月收集的基线数据显示,患者到达后评估存在显著延误。2013年和2014年开展了分诊培训课程并对质量改进工具进行了监测。实施障碍导致建造了一个独立的产科分诊亭,该分诊亭于2015年1月启用,配备了专门的助产士。在分诊亭启用后的三个时间间隔收集数据,并与基线数据进行比较,包括:转诊指征、患者和分娩特征、从到达至评估的等待时间以及护理计划的记录。在为期5年的干预期间,一项产科分诊改善计划将从设施到达至由助产士进行首次评估的患者中位(四分位间距)等待时间从40分钟(15 - 100分钟)减少至5分钟(2 - 6分钟)(p<0.001)。分诊亭提高了绩效,消除了先前与入院时间和疾病严重程度相关的延误。护理计划记录从51%增加到了96%。产科分诊若得到妥善实施,可减少繁忙的资源匮乏医院中的延误。在向新医院过渡期间,实施过程在当地领导下得以持续。