Department of Radiation Oncology, Cancer Centre Amsterdam, Academic Medical Centre, Amsterdam, The Netherlands.
Department of Surgery, Cancer Centre Amsterdam, Academic Medical Centre, Amsterdam, The Netherlands.
Br J Surg. 2018 Jul;105(8):946-958. doi: 10.1002/bjs.10870. Epub 2018 Apr 30.
Studies comparing upfront surgery with neoadjuvant treatment in pancreatic cancer may report only patients who underwent resection and so survival will be skewed. The aim of this study was to report survival by intention to treat in a comparison of upfront surgery versus neoadjuvant treatment in resectable or borderline resectable pancreatic cancer.
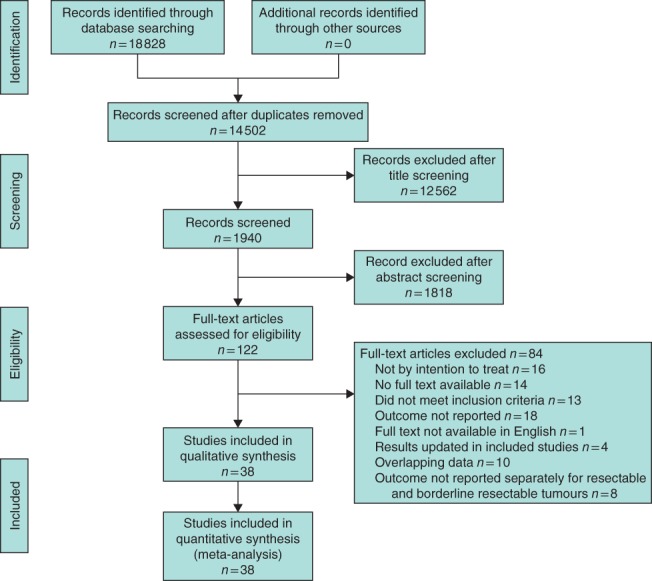
MEDLINE, Embase and the Cochrane Library were searched for studies reporting median overall survival by intention to treat in patients with resectable or borderline resectable pancreatic cancer treated with or without neoadjuvant treatment. Secondary outcomes included overall and R0 resection rate, pathological lymph node rate, reasons for unresectability and toxicity of neoadjuvant treatment.
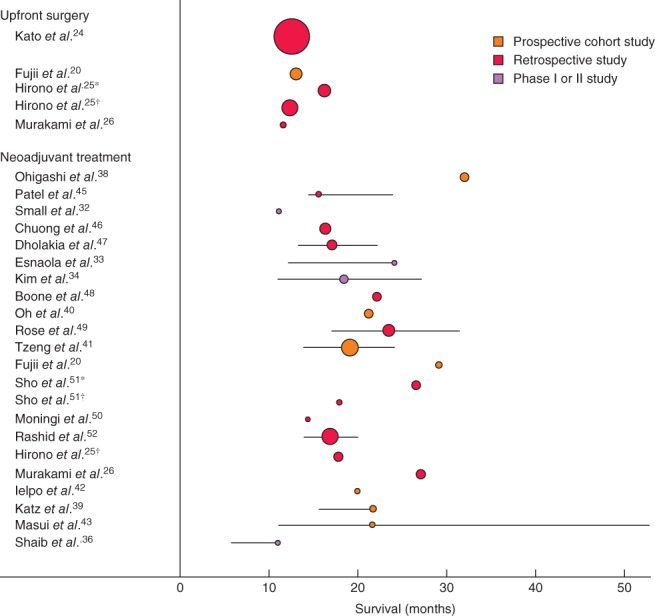
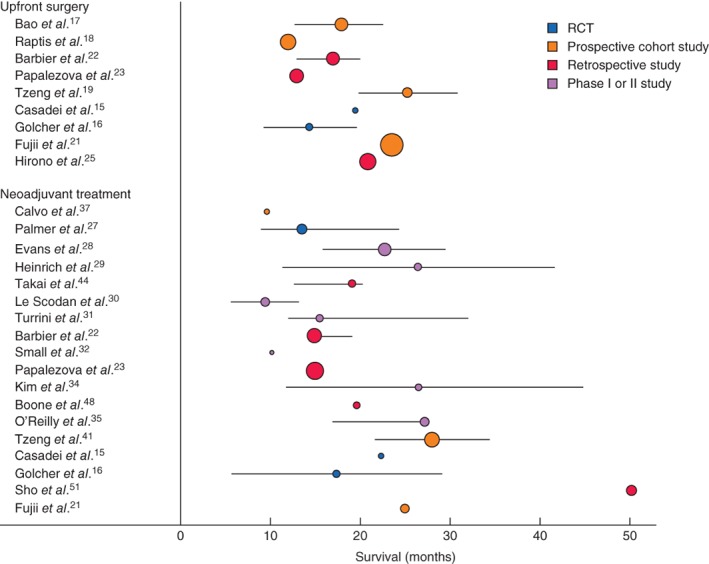
In total, 38 studies were included with 3484 patients, of whom 1738 (49·9 per cent) had neoadjuvant treatment. The weighted median overall survival by intention to treat was 18·8 months for neoadjuvant treatment and 14·8 months for upfront surgery; the difference was larger among patients whose tumours were resected (26·1 versus 15·0 months respectively). The overall resection rate was lower with neoadjuvant treatment than with upfront surgery (66·0 versus 81·3 per cent; P < 0·001), but the R0 rate was higher (86·8 (95 per cent c.i. 84·6 to 88·7) versus 66·9 (64·2 to 69·6) per cent; P < 0·001). Reported by intention to treat, the R0 rates were 58·0 and 54·9 per cent respectively (P = 0·088). The pathological lymph node rate was 43·8 per cent after neoadjuvant therapy and 64·8 per cent in the upfront surgery group (P < 0·001). Toxicity of at least grade III was reported in up to 64 per cent of the patients.
Neoadjuvant treatment appears to improve overall survival by intention to treat, despite lower overall resection rates for resectable or borderline resectable pancreatic cancer. PROSPERO registration number: CRD42016049374.
比较胰腺癌直接手术与新辅助治疗的研究可能只报告接受切除术的患者,因此生存情况会存在偏倚。本研究旨在报告可切除或交界可切除胰腺癌患者接受直接手术与新辅助治疗比较的意向治疗生存情况。
检索 MEDLINE、Embase 和 Cochrane 图书馆,以报告可切除或交界可切除胰腺癌患者接受或不接受新辅助治疗的意向治疗中位总生存期的研究。次要结局包括总体和 RO 切除率、病理淋巴结率、不可切除的原因和新辅助治疗的毒性。
共纳入 38 项研究,共 3484 例患者,其中 1738 例(49.9%)接受了新辅助治疗。意向治疗的加权中位总生存期,新辅助治疗为 18.8 个月,直接手术为 14.8 个月;在肿瘤切除的患者中,差异更大(分别为 26.1 和 15.0 个月)。新辅助治疗的总体切除率低于直接手术(分别为 66.0%和 81.3%;P<0.001),但 RO 率更高(分别为 86.8%(95%可信区间 84.6 至 88.7)和 66.9%(64.2 至 69.6);P<0.001)。意向治疗报告的 RO 率分别为 58.0%和 54.9%(P=0.088)。新辅助治疗后的病理淋巴结率为 43.8%,直接手术组为 64.8%(P<0.001)。报告至少为 3 级的毒性反应的患者占比高达 64%。
尽管可切除或交界可切除胰腺癌的总体切除率较低,但新辅助治疗似乎可以提高意向治疗的总生存期。PROSPERO 注册号:CRD42016049374。