Queen Square Multiple Sclerosis Centre, UCL Institute of Neurology, Faculty of Brain Sciences, University College London, London, UK.
Centre for Medical Image Computing (CMIC), Department of Computer Science, University College London, UK.
Brain. 2018 Jun 1;141(6):1665-1677. doi: 10.1093/brain/awy088.
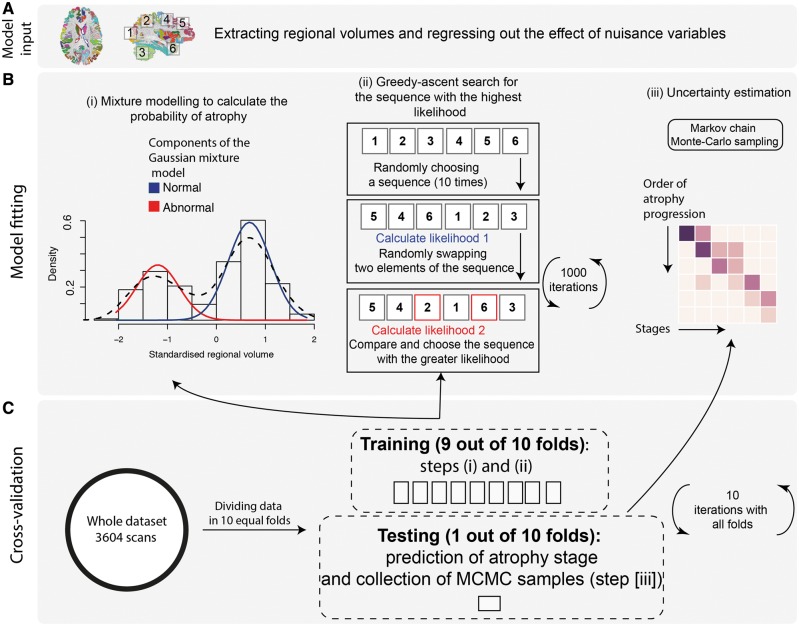
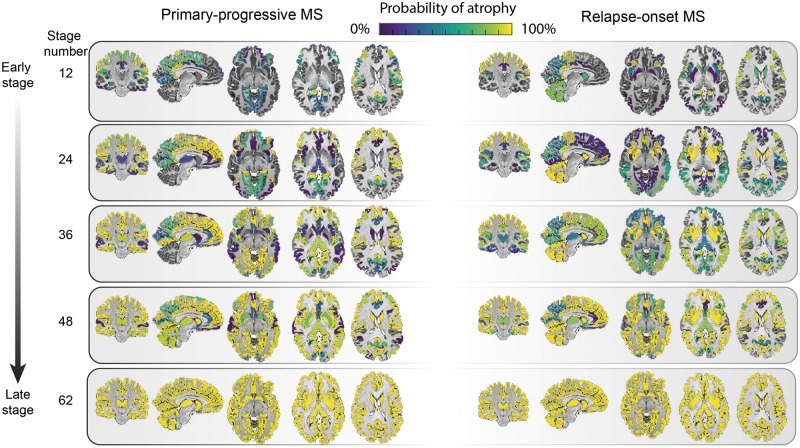
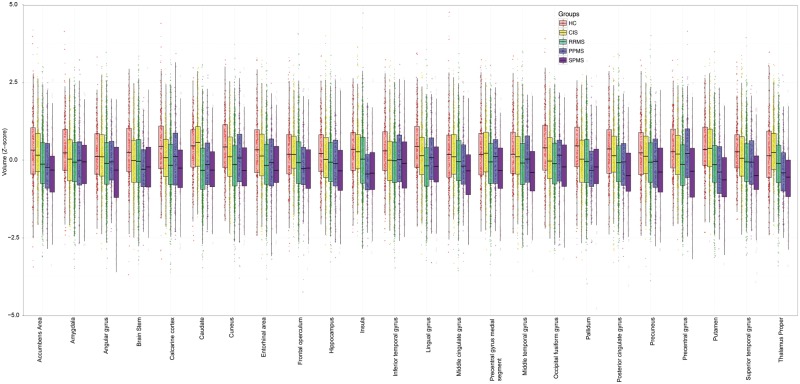
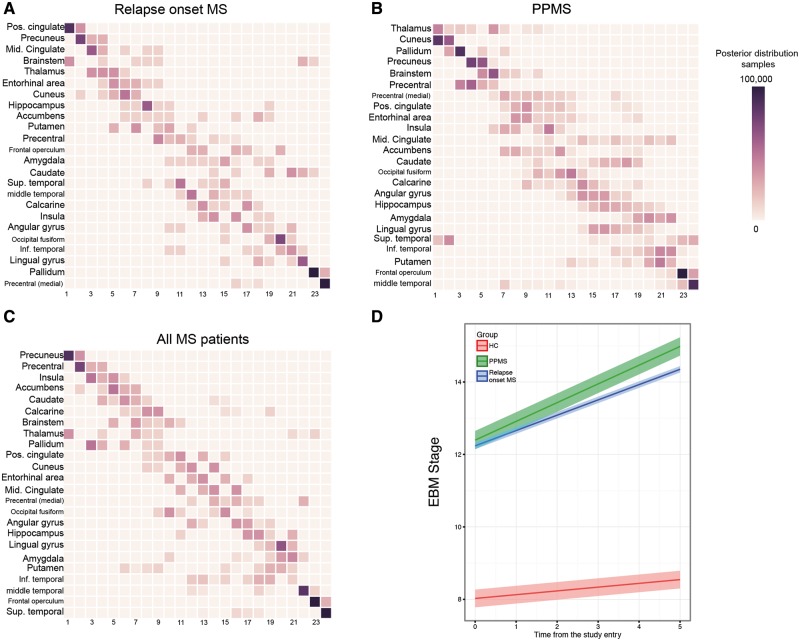
See Stankoff and Louapre (doi:10.1093/brain/awy114) for a scientific commentary on this article.Grey matter atrophy is present from the earliest stages of multiple sclerosis, but its temporal ordering is poorly understood. We aimed to determine the sequence in which grey matter regions become atrophic in multiple sclerosis and its association with disability accumulation. In this longitudinal study, we included 1417 subjects: 253 with clinically isolated syndrome, 708 with relapsing-remitting multiple sclerosis, 128 with secondary-progressive multiple sclerosis, 125 with primary-progressive multiple sclerosis, and 203 healthy control subjects from seven European centres. Subjects underwent repeated MRI (total number of scans 3604); the mean follow-up for patients was 2.41 years (standard deviation = 1.97). Disability was scored using the Expanded Disability Status Scale. We calculated the volume of brain grey matter regions and brainstem using an unbiased within-subject template and used an established data-driven event-based model to determine the sequence of occurrence of atrophy and its uncertainty. We assigned each subject to a specific event-based model stage, based on the number of their atrophic regions. Linear mixed-effects models were used to explore associations between the rate of increase in event-based model stages, and T2 lesion load, disease-modifying treatments, comorbidity, disease duration and disability accumulation. The first regions to become atrophic in patients with clinically isolated syndrome and relapse-onset multiple sclerosis were the posterior cingulate cortex and precuneus, followed by the middle cingulate cortex, brainstem and thalamus. A similar sequence of atrophy was detected in primary-progressive multiple sclerosis with the involvement of the thalamus, cuneus, precuneus, and pallidum, followed by the brainstem and posterior cingulate cortex. The cerebellum, caudate and putamen showed early atrophy in relapse-onset multiple sclerosis and late atrophy in primary-progressive multiple sclerosis. Patients with secondary-progressive multiple sclerosis showed the highest event-based model stage (the highest number of atrophic regions, P < 0.001) at the study entry. All multiple sclerosis phenotypes, but clinically isolated syndrome, showed a faster rate of increase in the event-based model stage than healthy controls. T2 lesion load and disease duration in all patients were associated with increased event-based model stage, but no effects of disease-modifying treatments and comorbidity on event-based model stage were observed. The annualized rate of event-based model stage was associated with the disability accumulation in relapsing-remitting multiple sclerosis, independent of disease duration (P < 0.0001). The data-driven staging of atrophy progression in a large multiple sclerosis sample demonstrates that grey matter atrophy spreads to involve more regions over time. The sequence in which regions become atrophic is reasonably consistent across multiple sclerosis phenotypes. The spread of atrophy was associated with disease duration and with disability accumulation over time in relapsing-remitting multiple sclerosis.
请参阅 Stankoff 和 Louapre 的科学评论(doi:10.1093/brain/awy114)。灰质萎缩存在于多发性硬化症的早期阶段,但它的时间顺序尚不清楚。我们旨在确定多发性硬化症中灰质区域萎缩的顺序及其与残疾积累的关系。在这项纵向研究中,我们纳入了来自七个欧洲中心的 1417 名受试者:253 名患有临床孤立综合征,708 名患有复发缓解型多发性硬化症,128 名患有继发进展型多发性硬化症,125 名患有原发进展型多发性硬化症,203 名健康对照者。受试者接受了重复的 MRI(共进行了 3604 次扫描);患者的平均随访时间为 2.41 年(标准差=1.97)。残疾使用扩展残疾状态量表进行评分。我们使用无偏的个体内模板计算了脑灰质区域和脑干的体积,并使用既定的数据驱动事件模型来确定萎缩的发生顺序及其不确定性。我们根据患者的萎缩区域数量,将每个患者分配到特定的基于事件的模型阶段。使用线性混合效应模型来探索基于事件的模型阶段增加率与 T2 病变负荷、疾病修正治疗、合并症、疾病持续时间和残疾积累之间的关联。在临床孤立综合征和复发发作型多发性硬化症患者中,首先发生萎缩的区域是后扣带回皮质和楔前叶,其次是中扣带回皮质、脑干和丘脑。原发性进行性多发性硬化症也检测到类似的萎缩顺序,涉及丘脑、楔前叶、楔叶和苍白球,其次是脑干和后扣带回皮质。小脑、尾状核和壳核在复发发作型多发性硬化症中较早发生萎缩,在原发性进行性多发性硬化症中较晚发生萎缩。继发性进行性多发性硬化症患者在研究开始时具有最高的基于事件的模型阶段(最高数量的萎缩区域,P<0.001)。所有多发性硬化症表型,但临床孤立综合征,均显示出比健康对照组更快的基于事件的模型阶段增加率。所有患者的 T2 病变负荷和疾病持续时间均与基于事件的模型阶段增加有关,但未观察到疾病修正治疗和合并症对基于事件的模型阶段的影响。基于事件的模型阶段的年化率与复发缓解型多发性硬化症的残疾积累有关,与疾病持续时间无关(P<0.0001)。在大型多发性硬化症样本中,基于数据驱动的萎缩进展分期表明,灰质萎缩随着时间的推移向更多区域扩散。各多发性硬化症表型之间萎缩区域的发生顺序相当一致。萎缩的扩散与疾病持续时间以及复发缓解型多发性硬化症中随时间推移的残疾积累有关。