Division of Cancer and Genetics, Cardiff University, University Hospital of Wales, Heath Park, Cardiff, Wales, UK.
Department of Surgery, Cardiff & Vale University Health Board, Cardiff, Wales, UK.
J Gastrointest Surg. 2018 Sep;22(9):1516-1527. doi: 10.1007/s11605-018-3787-9. Epub 2018 May 15.
Survival and relapse after gastric cancer surgery are largely attributed to tumor biology and surgical radicality; yet, other prognostic factors have been reported, including respiratory sepsis and anastomotic leakage, but not global morbidity severity score (MSS). The hypothesis tested was that MSS would be associated with both disease-free (DFS) and overall survival (OS).
Consecutive 373 patients undergoing potentially curative surgery for gastric adenocarcinoma between 2004 and 2016 in a UK cancer network were studied. Complications were defined prospectively as any deviation from a pre-determined post-operative course within 30 days of surgery and classified according to the Clavien-Dindo severity classification (CDSC). Primary outcome measures were DFS and OS.
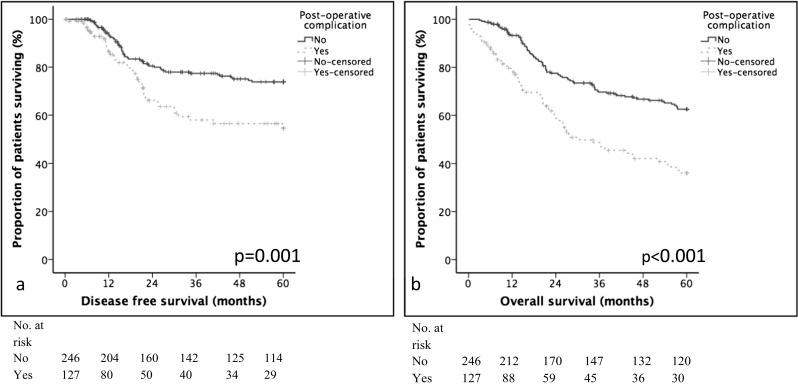
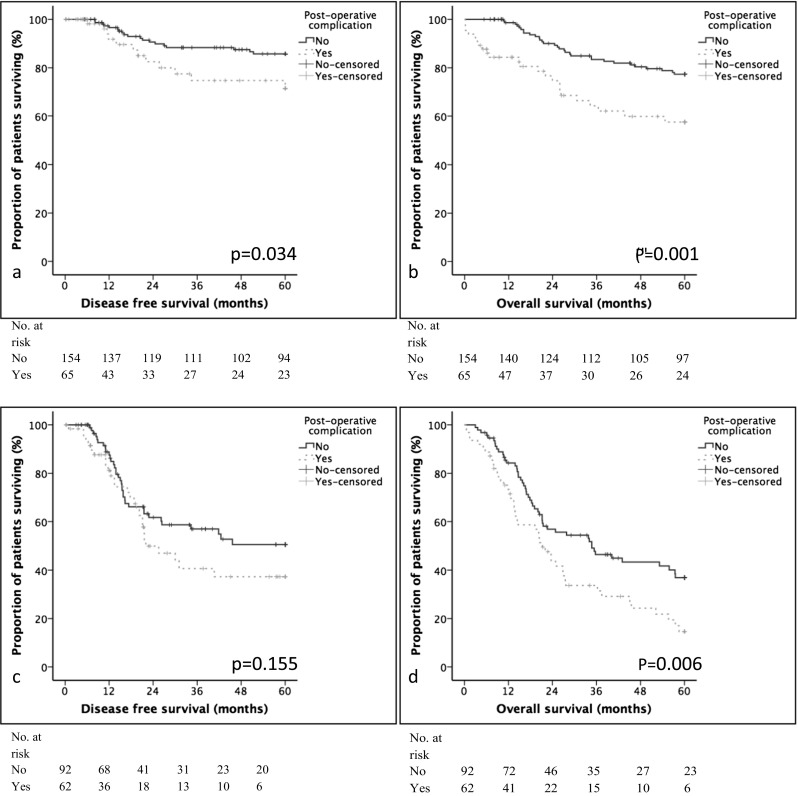
Post-operative complications were identified in 127 (34.0%) patients, which was associated with 9 (2.4%) post-operative deaths. Five-year DFS and OS were 35.9 and 38.5% for patients with a post-operative complication compared with 59.5 and 61.5% in controls (p < 0.001, p = 0.001, respectively). On multivariable DFS analysis, post-operative morbidity [hazard ratio (HR) 1.63, 95% confidence interval (CI) 1.06-2.50, p = 0.026] was independently associated with poor survival. On multivariable OS analysis, post-operative morbidity HR 2.25 (95% CI 1.04-4.85, p = 0.039) and CDSC HR 1.76 (95% CI 1.35-2.29, p < 0.001) were independently associated with poor survival. These associations were also observed in patients with TNM stage I and II disease with morbidity HR 7.06 (95% CI 1.89-26.38, p = 0.004) and CDSC HR 2.93 (95% CI 1.89-4.55, p < 0.001) offering independent prognostic value.
Post-operative CDSC was an important independent prognostic factor after potentially curative gastrectomy for carcinoma associated with both DFS and OS. Prehabilitation strategies to minimize complications are warranted.
胃癌手术后的生存和复发主要归因于肿瘤生物学和手术根治性;然而,已经报道了其他预后因素,包括呼吸性败血症和吻合口漏,但不包括全球发病率严重程度评分(MSS)。测试的假设是 MSS 将与无病生存期(DFS)和总生存期(OS)相关。
在英国癌症网络中,对 2004 年至 2016 年间接受潜在根治性手术治疗的 373 例胃腺癌患者进行了连续研究。并发症前瞻性定义为手术 30 天内与预定术后过程的任何偏差,并根据 Clavien-Dindo 严重程度分类(CDSC)进行分类。主要结局指标是 DFS 和 OS。
127 例(34.0%)患者发生术后并发症,其中 9 例(2.4%)术后死亡。术后并发症患者的 5 年 DFS 和 OS 分别为 35.9%和 38.5%,而对照组为 59.5%和 61.5%(p<0.001,p=0.001)。多变量 DFS 分析显示,术后发病率[风险比(HR)1.63,95%置信区间(CI)1.06-2.50,p=0.026]与不良生存相关。多变量 OS 分析显示,术后发病率 HR 2.25(95%CI 1.04-4.85,p=0.039)和 CDSC HR 1.76(95%CI 1.35-2.29,p<0.001)与不良生存相关。这些关联在 TNM 分期 I 和 II 期疾病患者中也观察到,发病率 HR 7.06(95%CI 1.89-26.38,p=0.004)和 CDSC HR 2.93(95%CI 1.89-4.55,p<0.001)提供了独立的预后价值。
术后 CDSC 是与 DFS 和 OS 相关的潜在根治性胃切除术后的重要独立预后因素。需要采取预康复策略来最大程度地减少并发症。