Department of Biomedical Informatics, The University of Tokyo, 7-3-1 Hongo, Bunkyo, Tokyo, 113-0033, Japan.
Division of Health Policy and Management, Center for Community Medicine, Jichi Medical University, 3311-1 Yakushiji, Shimotsuke, Tochigi, 329-0498, Japan.
Int J Health Geogr. 2018 May 21;17(1):13. doi: 10.1186/s12942-018-0133-0.
Coronary computed tomography angiography (CTA) has demonstrated high diagnostic accuracy for detection of coronary artery stenosis, and healthcare providers can detect coronary artery disease in earlier stages before it develops into more serious clinical conditions such as acute myocardial infarction (AMI). We hypothesized that the mortality ratio of AMI in regions with a higher density of coronary CTA is lower than that in regions with a lower density of coronary CTA.
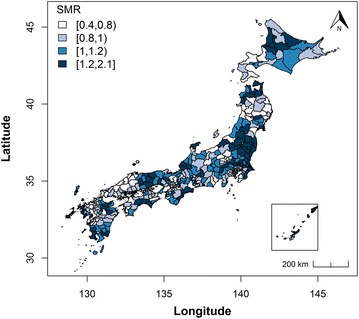
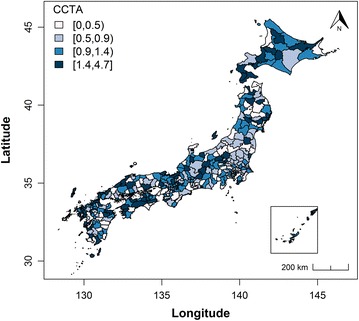
This ecological and cross-sectional study using secondary data targeted all secondary medical service areas (SMSAs) in Japan (n = 349). We obtained the numbers of cardiologists, institutions with coronary CTA, and institutions with a cardiac catheterization laboratory (CCL) as medical resources, socioeconomic factors, lifestyle factors, exercise habit factors, and AMI mortality data from a Japanese national database. We evaluated the association between the number of these medical resources and the standardized mortality ratio (SMR) of AMI in each SMSA using a hierarchical Bayesian model accounting for spatial autocorrelation (i.e., a conditional autoregressive model). We assumed a Poisson distribution for the observed number of AMI-related deaths and set the expected number of AMI-related deaths as the offset variable.
The number of institutions with coronary CTA was negatively and significantly associated with the SMR of AMI (relative risk [RR] 0.900; 95% credible interval [CI] 0.848-0.953), while the SMR in each SMSA was not significantly associated with the number of either cardiologists (RR 0.997; 95% CI 0.988-1.004) or institutions with a CCL (RR 1.026; 95% CI 0.963-1.096).
We observed a significant association between the number of institutions with coronary CTA and the SMR of AMI. Effective allocation of coronary CTA in each region is recommended, and it would be important to clarify the standing position of coronary CTA in regional networking for AMI treatment in the future.
冠状动脉计算机断层血管造影(CTA)在检测冠状动脉狭窄方面具有较高的诊断准确性,医疗服务提供者可以在冠状动脉疾病发展为更严重的临床病症(如急性心肌梗死(AMI))之前的早期阶段检测到该疾病。我们假设,冠状动脉 CTA 密度较高的地区的 AMI 死亡率低于冠状动脉 CTA 密度较低的地区。
本研究使用二次数据进行了生态交叉研究,目标是日本所有二级医疗服务区(SMSA)(n=349)。我们从日本国家数据库中获得了心脏病专家数量、具有冠状动脉 CTA 的机构以及具有心脏导管插入术实验室(CCL)的机构数量等医疗资源数据,以及社会经济因素、生活方式因素、运动习惯因素和 AMI 死亡率数据。我们使用分层贝叶斯模型(考虑空间自相关,即条件自回归模型)评估了每个 SMSA 中这些医疗资源数量与 AMI 标准化死亡率(SMR)之间的关联。我们假设观察到的与 AMI 相关的死亡人数服从泊松分布,并将与 AMI 相关的死亡人数的预期数量设置为偏移变量。
具有冠状动脉 CTA 的机构数量与 AMI 的 SMR 呈负相关且具有统计学意义(相对风险[RR]0.900;95%可信区间[CI]0.848-0.953),而每个 SMSA 的 SMR 与心脏病专家数量(RR0.997;95%CI0.988-1.004)或具有 CCL 的机构数量(RR1.026;95%CI0.963-1.096)均无显著相关性。
我们观察到具有冠状动脉 CTA 的机构数量与 AMI 的 SMR 之间存在显著关联。建议在每个地区有效分配冠状动脉 CTA,并在未来阐明冠状动脉 CTA 在区域联网治疗 AMI 中的地位将是很重要的。