Williams Phoebe C M, Berkley James A
a Nuffield Department of Clinical Medicine , The University of Oxford , Oxford , UK.
b Kenya Medical Research Institute (KEMRI)/Wellcome Trust Research Programme , Kilifi , Kenya.
Paediatr Int Child Health. 2018 Nov;38(sup1):S50-S65. doi: 10.1080/20469047.2017.1409454.
Shigella remains the primary cause of diarrhoea in paediatric patients worldwide and accounts for up to 40,000 deaths per year. Current guidelines for the treatment of shigellosis are based on data which are over a decade old. In an era of increasing antimicrobial resistance, an updated review of the appropriate empirical therapy for shigellosis in children is necessary, taking into account susceptibility patterns, cost and the risk of adverse events.
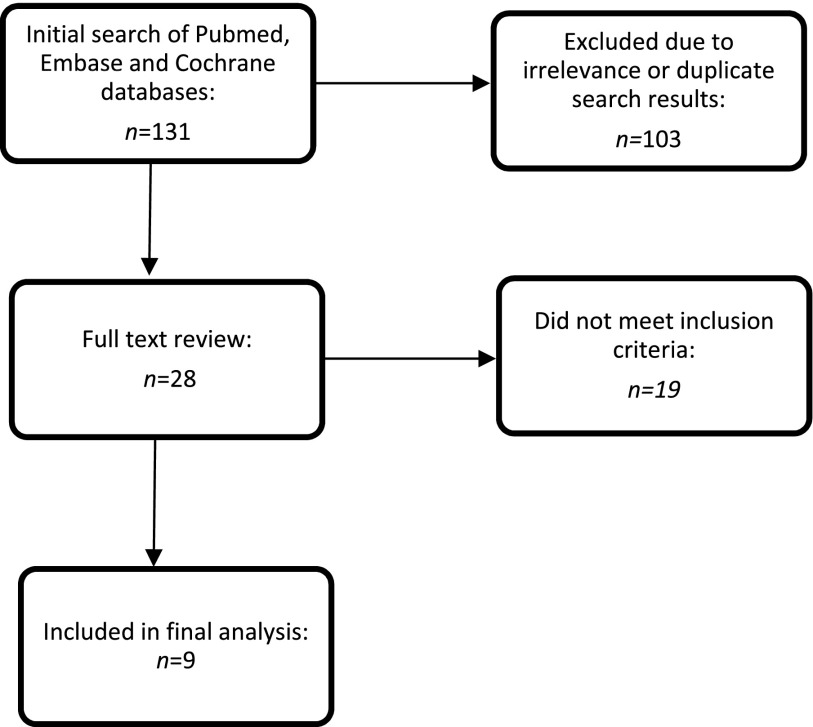
A systematic review of the current published literature on the treatment of shigella dysentery was undertaken in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
The initial search produced 131 results, of which nine studies met the inclusion criteria. The quality of the studies was assessed as per the Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidelines. International guidelines were also reviewed. There is a lack of current research regarding the clinical treatment of shigellosis in paediatric and adult patients, despite rising antimicrobial resistance worldwide. In particular, there is a lack of studies assessing the non-susceptibility of community-acquired strains, with almost all published research pertaining to microbiological data from hospital-based settings.
Current WHO guidelines support the use of fluoroquinolones (first-line), β-lactams (second-line) and cephalosporins (second-line) which accords with currently available evidence and other international guidelines, and there is no strong evidence for changing this guidance. Azithromycin is appropriate as a second-line therapy in regions where the rate of non-susceptibility of ciprofloxacin is known to be high, and research suggests that, from a cardiac point of view, azithromycin is safer than other macrolide antibiotics. Cefixime is also a reasonable alternative, although its use must be weighed against the risk of dissemination of extended-spectrum β-lactamase-producing organisms.
志贺氏菌仍然是全球儿科患者腹泻的主要病因,每年导致多达4万例死亡。目前的志贺氏菌病治疗指南所依据的数据已有十多年历史。在抗菌药物耐药性不断增加的时代,有必要对儿童志贺氏菌病的适当经验性治疗进行更新回顾,同时考虑药敏模式、成本和不良事件风险。
根据系统评价和Meta分析的首选报告项目(PRISMA),对目前已发表的关于志贺氏菌痢疾治疗的文献进行系统评价。
初步检索产生了131条结果,其中9项研究符合纳入标准。根据推荐分级评估、制定和评价(GRADE)指南对研究质量进行评估。还对国际指南进行了回顾。尽管全球抗菌药物耐药性不断上升,但目前缺乏关于儿科和成人患者志贺氏菌病临床治疗的研究。特别是,缺乏评估社区获得性菌株不敏感性的研究,几乎所有已发表的研究都与来自医院环境的微生物学数据有关。
世界卫生组织目前的指南支持使用氟喹诺酮类(一线)、β-内酰胺类(二线)和头孢菌素类(二线),这与现有证据和其他国际指南一致,并且没有强有力的证据改变这一指导意见。在已知环丙沙星不敏感率较高的地区,阿奇霉素作为二线治疗是合适的,而且研究表明,从心脏方面来看,阿奇霉素比其他大环内酯类抗生素更安全。头孢克肟也是一种合理的替代药物,但其使用必须权衡产超广谱β-内酰胺酶生物传播的风险。