Department of General Internal Medicine, Fukushima Medical University, Fukushima, Japan.
Department of Clinical Medicine, Institute of Tropical Medicine, Nagasaki University, Nagasaki, Japan.
BMC Pulm Med. 2018 May 23;18(1):88. doi: 10.1186/s12890-018-0648-y.
Mortality prediction of pneumonia by severity scores in patients with multiple underlying health conditions has not fully been investigated. This prospective cohort study is to identify mortality-associated underlying health conditions and to analyse their influence on severity-based pneumonia mortality prediction.
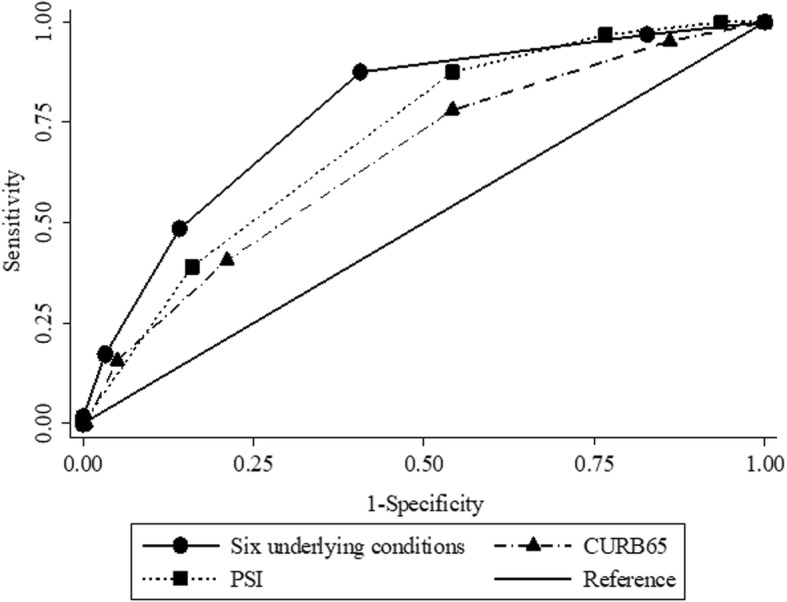
Adult patients with community-acquired pneumonia or healthcare-associated pneumonia (HCAP) who visited four community hospitals between September 2011 and January 2013 were enrolled. Candidate underlying health conditions, including demographic and clinical characteristics, were incorporated into the logistic regression models, along with CURB (confusion, elevated urea nitrogen, tachypnoea, and hypotension) score as a measure of disease severity. The areas under the receiver operating characteristic curves (AUROC) of the predictive index based on significant underlying health conditions was compared to that of CURB65 (CURB and age ≥ 65) score or Pneumonia severity index (PSI). Mortality association between disease severity and the number of underlying health conditions was analysed.
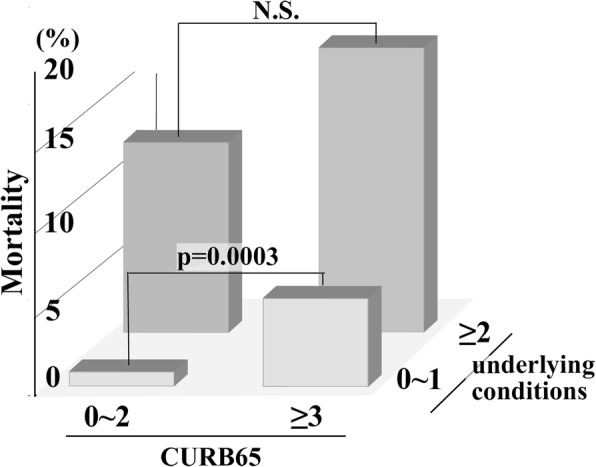
In total 1772 patients were eligible for analysis, of which 140 (7.9%) died within 30 days. Six underlying health conditions were independently associated: home care (adjusted odds ratio, 5.84; 95% confidence interval, CI, 2.28-14.99), recent hospitalization (2.21; 1.36-3.60), age ≥ 85 years (2.15; 1.08-4.28), low body mass index (1.99, 1.25-3.16), neoplastic disease (1.82; 1.17-2.85), and male gender (1.78; 1.16-2.75). The predictive index based on these conditions alone had a significantly or marginally higher AUROC than that based on CURB65 score (0.78 vs 0.66, p = 0.02) or PSI (0.78 vs 0.71, p = 0.05), respectively. Compared to this index, the AUROC of the total score consisting of six underlying health conditions and CURB score (range 0-10) did not improve mortality predictions (p = 0.3). In patients with one or less underlying health conditions, the mortality was discretely associated with severe pneumonia (CURB65 ≥ 3) (risk ratio: 7.24, 95%CI: 3.08-25.13), whereas in patients with 2 or more underlying health conditions, the mortality association with severe pneumonia was not detected (risk ratio: 1.53, 95% CI: 0.94-2.50).
Mortality prediction based on pneumonia severity scores is highly influenced by the accumulating number of underlying health conditions in an ageing society. The validation using a different cohort is necessary to generalise the conclusion.
在患有多种基础健康状况的患者中,使用严重程度评分预测肺炎死亡率尚未得到充分研究。本前瞻性队列研究旨在确定与死亡率相关的基础健康状况,并分析它们对基于严重程度的肺炎死亡率预测的影响。
2011 年 9 月至 2013 年 1 月期间,在四家社区医院就诊的患有社区获得性肺炎或医疗保健相关性肺炎(HCAP)的成年患者被纳入研究。候选基础健康状况,包括人口统计学和临床特征,被纳入逻辑回归模型中,同时还纳入 CURB(意识障碍、尿素氮升高、呼吸急促和低血压)评分作为疾病严重程度的衡量标准。基于显著基础健康状况的预测指标的受试者工作特征曲线(ROC)下面积(AUROC)与 CURB65(CURB 和年龄≥65 岁)评分或肺炎严重指数(PSI)进行比较。分析疾病严重程度与基础健康状况数量之间的死亡率相关性。
共有 1772 名患者符合分析条件,其中 140 名(7.9%)在 30 天内死亡。六个基础健康状况独立相关:家庭护理(调整后的优势比,5.84;95%置信区间,CI,2.28-14.99)、近期住院(2.21;1.36-3.60)、年龄≥85 岁(2.15;1.08-4.28)、低体重指数(1.99,1.25-3.16)、肿瘤疾病(1.82;1.17-2.85)和男性(1.78;1.16-2.75)。仅基于这些条件的预测指标的 AUROC 显著或略有高于基于 CURB65 评分(0.78 与 0.66,p=0.02)或 PSI(0.78 与 0.71,p=0.05)的 AUROC。与该指标相比,由六个基础健康状况和 CURB 评分组成的总分(范围 0-10)的 AUROC 并不能改善死亡率预测(p=0.3)。在患有一个或更少基础健康状况的患者中,死亡率与严重肺炎(CURB65≥3)明显相关(风险比:7.24,95%CI:3.08-25.13),而在患有两个或更多基础健康状况的患者中,严重肺炎与死亡率之间的相关性未被检测到(风险比:1.53,95%CI:0.94-2.50)。
基于肺炎严重程度评分的死亡率预测受老龄化社会中基础健康状况数量的累积影响较大。使用不同队列进行验证对于推广该结论是必要的。