Department of Radiation Oncology, University Hospital Johann Wolfgang Goethe University, Frankfurt, Germany.
Saphir Radiosurgery Center, Frankfurt, Germany.
PLoS One. 2018 Jun 6;13(6):e0198692. doi: 10.1371/journal.pone.0198692. eCollection 2018.
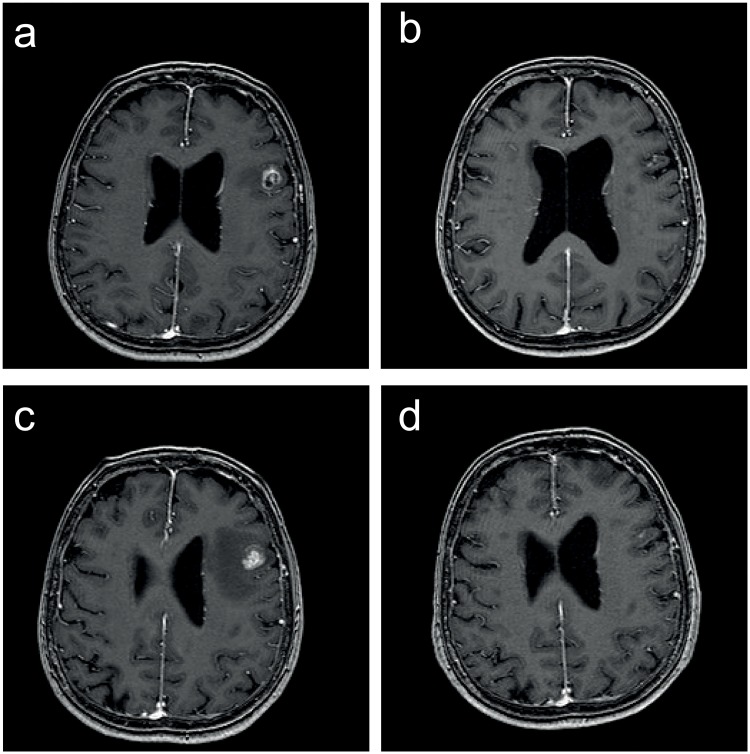
Stereotactic radiosurgery (SRS) is an established primary treatment for newly diagnosed brain metastases with high local control rates. However, data about local re-irradiation in case of local failure after SRS (re-SRS) are rare. We evaluated the feasibility, efficacy and patient selection characteristics in treating locally recurrent metastases with a second course of SRS.
We retrospectively evaluated patients with brain metastases treated with re-SRS for local tumor progression between 2011 and 2017. Patient and treatment characteristics as well as rates of tumor control, survival and toxicity were analyzed.
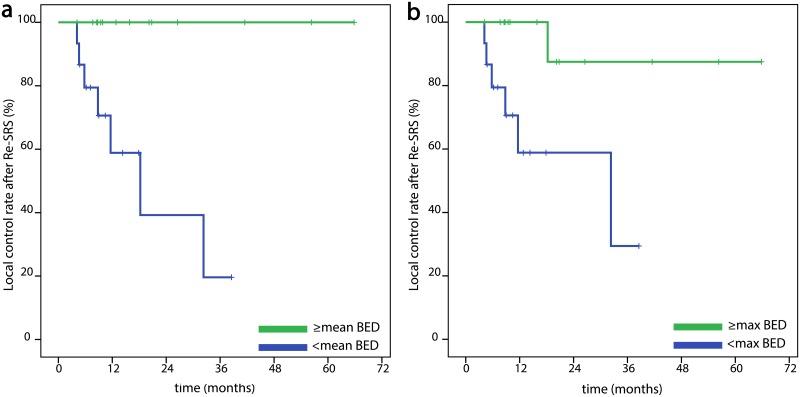
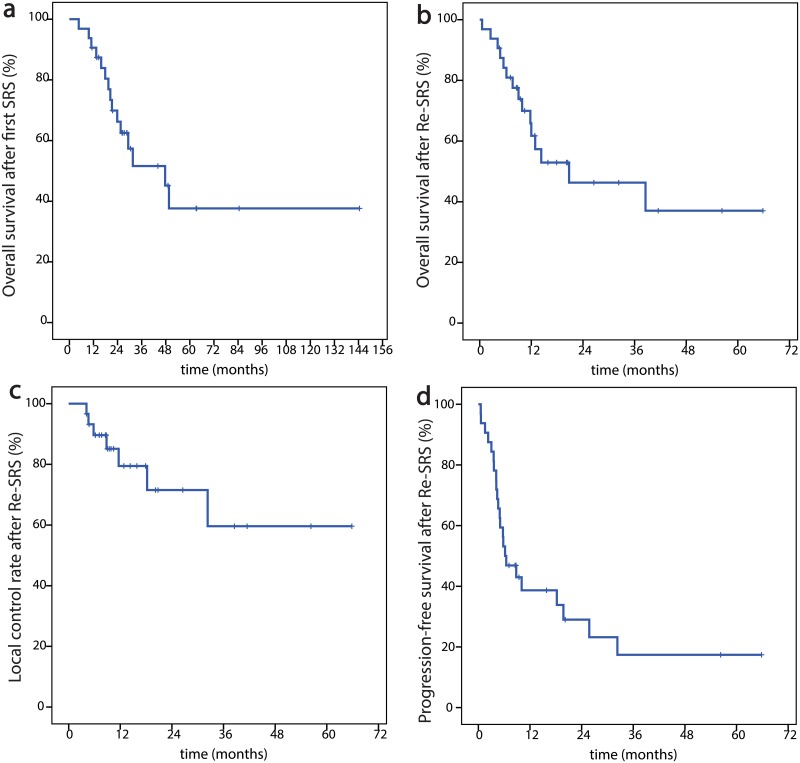
Overall, 32 locally recurrent brain metastases in 31 patients were irradiated with re-SRS. Median age at re-SRS was 64.9 years. The primary histology was breast cancer and non-small-cellular lung cancer (NSCLC) in respectively 10 cases (31.3%), in 5 cases malignant melanoma (15.6%). In the first SRS-course 19 metastases (59.4%) and in the re-SRS-course 29 metastases (90.6%) were treated with CyberKnife® and the others with Gamma Knife. Median planning target volume (PTV) for re-SRS was 2.5 cm3 (range, 0.1-37.5 cm3) and median dose prescribed to the PTV was 19 Gy (range, 12-28 Gy) in 1-5 fractions to the median 69% isodose (range, 53-80%). The 1-year overall survival rate was 61.7% and the 1-year local control rate was 79.5%. The overall rate of radiological radio-necrosis was 16.1% and four patients (12.9%) experienced grade ≥ 3 toxicities.
A second course of SRS for locally recurrent brain metastases after prior local SRS appears to be feasible with acceptable toxicity and can be considered as salvage treatment option for selected patients with high performance status. Furthermore, this is the first study utilizing robotic radiosurgery for this indication, as an additional option for frameless fractionated treatment.
立体定向放射外科(SRS)是治疗新诊断的脑转移瘤的一种既定的主要治疗方法,具有较高的局部控制率。然而,关于 SRS 后局部失败(再 SRS)时局部再照射的数据很少。我们评估了在 SRS 后局部复发的情况下,用第二疗程 SRS 治疗局部复发转移的可行性、疗效和患者选择特征。
我们回顾性评估了 2011 年至 2017 年间因局部肿瘤进展而行再 SRS 治疗的脑转移瘤患者。分析了患者和治疗特征以及肿瘤控制、生存和毒性的发生率。
共有 31 例患者的 32 个局部复发脑转移瘤接受了再 SRS 治疗。再 SRS 时的中位年龄为 64.9 岁。原发组织学为乳腺癌和非小细胞肺癌(NSCLC),分别为 10 例(31.3%)和 5 例(15.6%)。在首次 SRS 疗程中,19 个转移灶(59.4%)和再 SRS 疗程中,29 个转移灶(90.6%)采用 CyberKnife®治疗,其余采用伽玛刀治疗。再 SRS 的中位计划靶区(PTV)体积为 2.5 cm3(范围,0.1-37.5 cm3),中位 PTV 处方剂量为 19 Gy(范围,12-28 Gy),分为 1-5 个分次,达到中位数 69%等剂量线(范围,53-80%)。1 年总生存率为 61.7%,1 年局部控制率为 79.5%。总的放射性脑坏死发生率为 16.1%,4 名患者(12.9%)发生≥3 级毒性。
在先前的局部 SRS 后,对于局部复发的脑转移瘤进行第二次 SRS 似乎是可行的,具有可接受的毒性,并且可以作为选择高功能状态患者的挽救性治疗选择。此外,这是第一项利用机器人放射外科治疗该疾病的研究,为无框架分次治疗提供了另一种选择。