Marvasti Tina Binesh, Moody Alan R, Singh Navneet, Maraj Tishan, Tyrrell Pascal, Afshin Mariam
Institute of Medical Sciences, University of Toronto, Toronto, Ontario, Canada.
Department of Medical Imaging, University of Toronto, Toronto, Ontario, Canada.
Int J Cardiol Heart Vasc. 2017 Dec 6;18:96-100. doi: 10.1016/j.ijcha.2017.11.003. eCollection 2018 Mar.
Atherosclerotic intraplaque hemorrhage (IPH) is a source of free hemoglobin that binds the haptoglobin protein and forms a complex cleared by CD163 macrophages. Compared to the other common haptoglobin genotypes, hemoglobin-haptoglobin2-2 complex has the lowest affinity for tissue macrophages resulting in lower rate of hemoglobin uptake and increased oxidative burden. We hypothesized that haptoglobin2-2 patients' failure to clear hemoglobin results in a greater prevalence and progression of IPH.
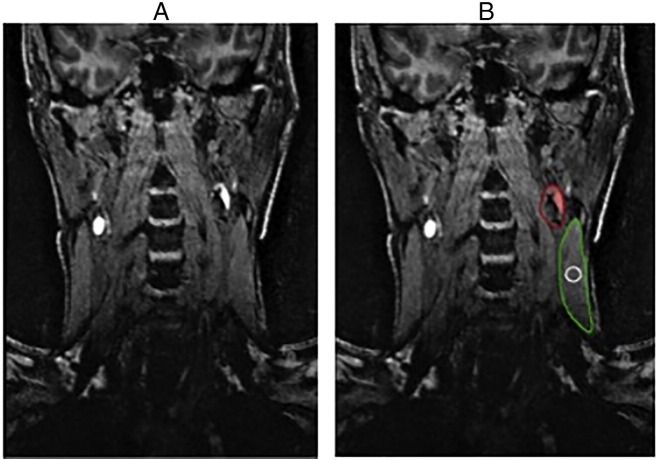
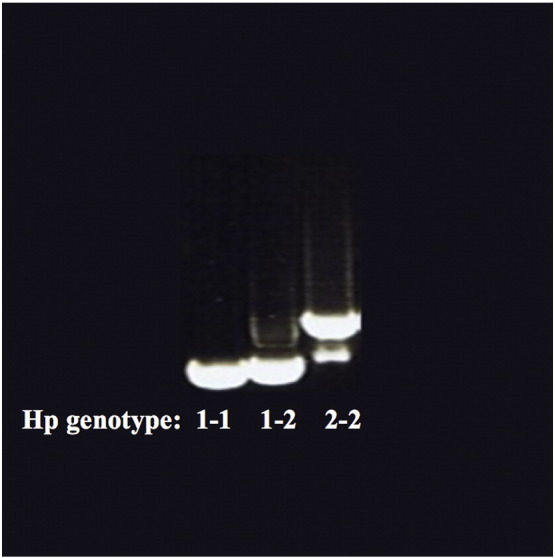
Prevalence and volume of IPH were measured in eighty patients with advanced vascular disease using MRI. Haptoglobin was genotyped using PCR. Mixed Models Repeated Measures Analyses were performed to detect any differences in prevalence and volume of IPH between the haptoglobin genotypes.
Haptoglobin2-2 patients had a statistically significant higher prevalence of baseline IPH (OR = 4.34, p-value: 0.01, 95% CI: 1.31-14.35). Longitudinal analysis of 48 IPH positive carotids indicated a statistically significant progression of IPH volume over time in haptoglobin2-2 patients (Type 3 test for fixed effect p-value = 0.0106; baseline vs. year 3: β = 0.11, SE = 0.05, p-value = 0.03; year 2 vs. year 3: β = 0.05, SE = 0.02, p-value = 0.03).
Patients with the Hp2-2 genotype had a significantly higher prevalence of carotid baseline IPH, which progressed over a two year follow up period. Detection of pre-symptomatic vascular disease using haptoglobin genotyping may allow for better risk stratification of populations at risk of stroke and in need of more targeted imaging investigations.
动脉粥样硬化斑块内出血(IPH)是游离血红蛋白的一个来源,游离血红蛋白与触珠蛋白结合形成复合物,该复合物由CD163巨噬细胞清除。与其他常见的触珠蛋白基因型相比,血红蛋白-触珠蛋白2-2复合物对组织巨噬细胞的亲和力最低,导致血红蛋白摄取率降低和氧化负担增加。我们推测,触珠蛋白2-2型患者清除血红蛋白的失败会导致IPH的更高患病率和进展。
使用MRI测量了80例晚期血管疾病患者的IPH患病率和体积。采用PCR对触珠蛋白进行基因分型。进行混合模型重复测量分析,以检测触珠蛋白基因型之间IPH患病率和体积的任何差异。
触珠蛋白2-2型患者基线IPH的患病率在统计学上显著更高(OR = 4.34,p值:0.01,95% CI:1.31 - 14.35)。对48条IPH阳性颈动脉的纵向分析表明,触珠蛋白2-2型患者的IPH体积随时间在统计学上有显著进展(固定效应的3型检验p值 = 0.0106;基线与第3年:β = 0.11,SE = 0.05,p值 = 0.03;第2年与第3年:β = 0.05,SE = 0.02,p值 = 0.03)。
Hp2-2基因型患者颈动脉基线IPH的患病率显著更高,且在两年的随访期内有所进展。使用触珠蛋白基因分型检测无症状血管疾病可能有助于对有中风风险且需要更有针对性的影像学检查的人群进行更好的风险分层。