Anesthesia and Intensive Care Department, Hôpitaux Universitaires Paris-Sud, Université Paris-Sud, Université Paris-Saclay, Hôpital De Bicêtre, Assistance Publique Hôpitaux de Paris (APHP), 78, Rue du Général Leclerc, 94270 Le Kremlin-Bicêtre, France.
Crit Care. 2018 Jun 15;22(1):161. doi: 10.1186/s13054-018-2067-0.
Renal perfusion status remains poorly studied at the bedside during septic shock. We sought to measure cortical renal perfusion in patients with septic shock during their first 3 days of care using renal contrast enhanced ultrasound (CEUS).
We prospectively included 20 ICU patients with septic shock and 10 control patients (CL) without septic shock admitted to a surgical ICU. Cortical renal perfusion was evaluated with CEUS during continuous infusion of Sonovue (Milan, Italy) within the first 24 h (day 0), between 24 and 48 h (day 1) and after 72 h (day 3) of care. Each measurement consisted of three destruction replenishment sequences that were recorded for delayed analysis with dedicated software (Vuebox). Renal perfusion was quantified by measuring the mean transit time (mTT) and the perfusion index (PI), which is the ratio of renal blood volume (rBV) to mTT.
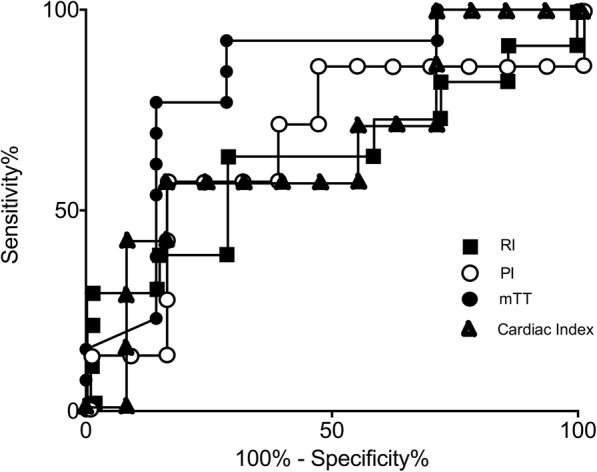
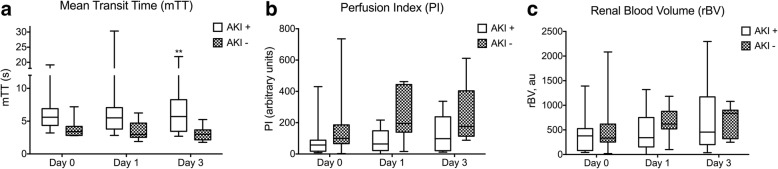
Cortical renal perfusion was decreased in septic shock as attested by a lower PI and a higher mTT in patients with septic shock than in patients of the CL group (p = 0.005 and p = 0.03). PI values had wider range in patients with septic shock (median (min-max) of 74 arbitrary units (a.u.) (3-736)) than in patients of the CL group 228 a.u. (67-440)). Renal perfusion improved over the first 3 days with a PI at day 3 higher than the PI at day 0 (74 (22-120) versus 160 (88-245) p = 0.02). mTT was significantly higher in patients with severe acute kidney injury (AKI) (n = 13) compared with patients with no AKI (n = 7) over time (p = 0.005). The PI was not different between patients with septic shock with severe AKI and those with no AKI (p = 0.29).
Although hemodynamic macrovascular parameters were restored, the cortical renal perfusion can be decreased, normal or even increased during septic shock. We observed an average decrease in cortical renal perfusion during septic shock compared to patients without septic shock. The decrease in cortical renal perfusion was associated with severe AKI occurrence. The use of renal CEUS to guide renal perfusion resuscitation needs further investigation.
在脓毒性休克期间,床边的肾脏灌注状态仍未得到很好的研究。我们试图使用肾脏对比增强超声(CEUS)在脓毒性休克患者接受治疗的前 3 天内测量皮质肾灌注。
我们前瞻性地纳入了 20 名 ICU 中患有脓毒性休克的患者和 10 名无脓毒性休克的对照患者(CL),这些患者被收治于外科 ICU。在接受 SonoVue(意大利米兰)连续输注的 24 小时内(第 0 天)、24 至 48 小时(第 1 天)和 72 小时(第 3 天)期间,使用 CEUS 评估皮质肾灌注。每个测量包括三个破坏再填充序列,使用专用软件(Vuebox)记录这些序列以供延迟分析。通过测量平均通过时间(mTT)和灌注指数(PI)来量化肾灌注,PI 是肾血容量(rBV)与 mTT 的比值。
脓毒性休克患者的皮质肾灌注降低,与 CL 组患者相比,脓毒性休克患者的 PI 较低,mTT 较高(p=0.005 和 p=0.03)。脓毒性休克患者的 PI 值范围较宽(中位数(最小值-最大值)为 74 个任意单位(a.u.)(3-736),而 CL 组患者为 228 a.u.(67-440))。在最初的 3 天内,肾灌注得到改善,第 3 天的 PI 高于第 0 天的 PI(74(22-120)比 160(88-245),p=0.02)。mTT 在有严重急性肾损伤(AKI)的患者(n=13)中明显高于没有 AKI 的患者(n=7)(p=0.005)。在脓毒性休克患者中,有严重 AKI 的患者与没有 AKI 的患者的 PI 没有差异(p=0.29)。
尽管宏观血流动力学参数得到恢复,但在脓毒性休克期间,皮质肾灌注可能会降低、正常甚至增加。与无脓毒性休克患者相比,我们观察到脓毒性休克期间皮质肾灌注平均降低。皮质肾灌注的降低与严重 AKI 的发生有关。使用肾脏 CEUS 来指导肾灌注复苏需要进一步研究。