Department of General Practice and Old Age Medicine, Amsterdam Public Health Research Institute, VU University Medical Center, Amsterdam, The Netherlands.
Dutch Association of Elderly Care Physicians, Utrecht, The Netherlands.
J Am Med Dir Assoc. 2018 Sep;19(9):757-764. doi: 10.1016/j.jamda.2018.05.001. Epub 2018 Jun 15.
Nonspecific signs and symptoms combined with positive urinalysis results frequently trigger antibiotic therapy in frail older adults. However, there is limited evidence about which signs and symptoms indicate urinary tract infection (UTI) in this population. We aimed to find consensus among an international expert panel on which signs and symptoms, commonly attributed to UTI, should and should not lead to antibiotic prescribing in frail older adults, and to integrate these findings into a decision tool for the empiric treatment of suspected UTI in this population.
A Delphi consensus procedure.
An international panel of practitioners recognized as experts in the field of UTI in frail older patients.
In 4 questionnaire rounds, the panel (1) evaluated the likelihood that individual signs and symptoms are caused by UTI, (2) indicated whether they would prescribe antibiotics empirically for combinations of signs and symptoms, and (3) provided feedback on a draft decision tool.
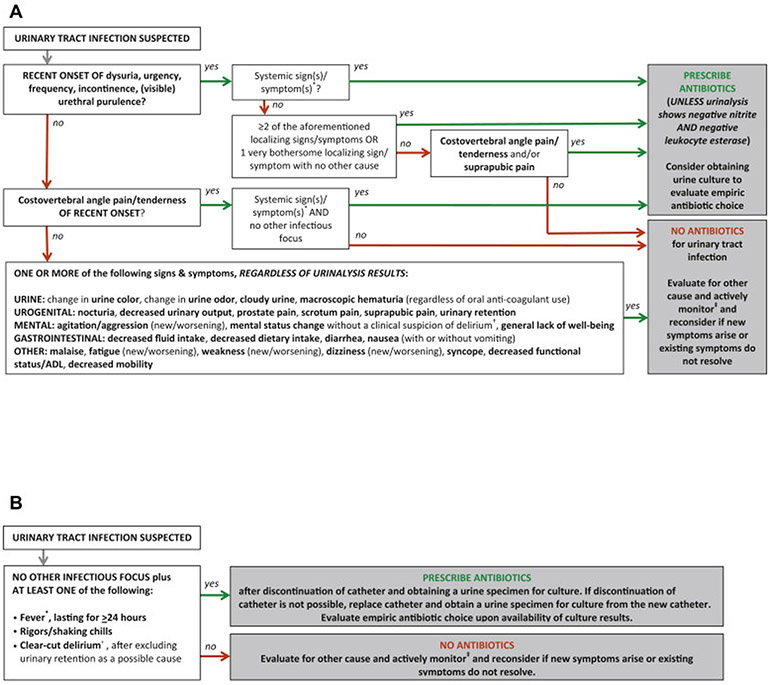
Experts agreed that the majority of nonspecific signs and symptoms should be evaluated for other causes instead of being attributed to UTI and that urinalysis should not influence treatment decisions unless both nitrite and leukocyte esterase are negative. These and other findings were incorporated into a decision tool for the empiric treatment for suspected UTI in frail older adults with and without an indwelling urinary catheter.
A decision tool for suspected UTI in frail older adults was developed based on consensus among an international expert panel. Studies are needed to evaluate whether this decision tool is effective in reaching its aim: the improvement of diagnostic evaluation and treatment for suspected UTI in frail older adults.
在体弱的老年人中,非特异性症状和体征结合阳性尿液分析结果常引发抗生素治疗。然而,关于哪些症状和体征提示该人群存在尿路感染(UTI)的证据有限。我们旨在让一个国际专家小组就哪些通常归因于 UTI 的症状和体征应该和不应该导致在体弱的老年人中开具抗生素达成共识,并将这些发现整合到一个针对该人群疑似 UTI 的经验性治疗的决策工具中。
德尔菲共识程序。
一个被认为是体弱老年患者 UTI 领域专家的国际从业者小组。
在 4 轮问卷中,专家组 (1) 评估了个体症状和体征由 UTI 引起的可能性,(2) 表示他们是否会根据症状和体征的组合经验性地开抗生素,(3) 对决策工具草案提供反馈。
专家们一致认为,大多数非特异性症状和体征应该评估其他原因,而不是归因于 UTI,并且除非亚硝酸盐和白细胞酯酶均为阴性,否则尿液分析不应影响治疗决策。这些发现和其他发现被纳入一个有和没有留置导尿管的体弱老年疑似 UTI 经验性治疗的决策工具中。
基于国际专家小组的共识,为体弱的老年人疑似 UTI 开发了一个决策工具。需要研究该决策工具是否能有效达到其目标:改善对体弱老年人疑似 UTI 的诊断评估和治疗。