Kim Tae-Hoon, Katsetos Manny, Dahal Khagendra, Azrin Michael, Lee Juyong
University of Connecticut Health Center, Connecticut, USA.
Sejong General Hospital, Bucheon, South Korea.
J Geriatr Cardiol. 2018 Apr;15(4):254-260. doi: 10.11909/j.issn.1671-5411.2018.04.006.
Development of arterial dissection is thought to be an important key factor for bailout stenting in femoropopliteal disease. We aimed to evaluate the difference in dissection rate and outcomes between the treatment group with rotational atherectomy and without it.
From January 2011 to October 2016, we compared the angiography after balloon angioplasty (BA) of de-novo, femoropopliteal, steno-occlusive lesions whether they were treated by rotational atherectomy prior to the BA or not. Fifty-nine lesions (8 occlusions; 3 involving popliteal segment; lesion length: 86.3 ± 66.8 mm) in 44 patients (29 males; mean age 66.9 ± 9.7 years) were enrolled for this review.
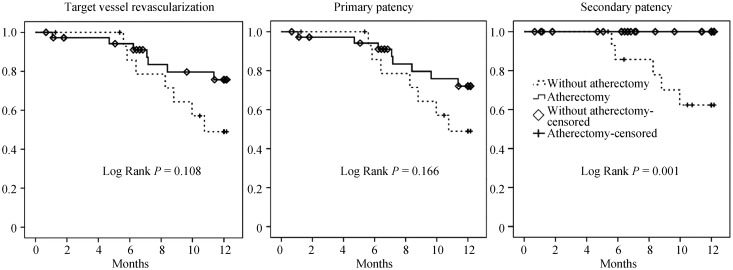
Forty-two lesions were treated using rotational atherectomy, prior to BA while 17 were recanalized firstly by BA. Clinical and lesion characteristics were not different between the groups. However, the rate of significant arterial dissection (type C to F) was lower in the atherectomy group (88.2% . 42.9%; = 0.001). In multivariate analysis, use of the atherectomy device was the only risk factor for prevention of development of significant dissection ( = 0.013; OR = 0.12; 95% CI: 0.025-0.642). Patients were treated either by the angioplasty alone, drug coated balloon or stent insertion. There was lower trend in target vessel revascularization and primary patency toward the atherectomy group (low rank = 0.108 and 0.166), however secondary patency was significantly better (low rank = 0.001).
Rotational atherectomy before BA reduced the rate of significant dissection and therefore, might be a valuable option for minimizing need of bailout stenting.
动脉夹层的发生被认为是股腘动脉疾病中补救性支架置入的一个重要关键因素。我们旨在评估旋磨术治疗组和未使用旋磨术治疗组之间夹层发生率及预后的差异。
2011年1月至2016年10月,我们比较了初发的股腘动脉狭窄闭塞性病变在球囊血管成形术(BA)前是否接受旋磨术治疗后的血管造影情况。本研究纳入了44例患者(29例男性;平均年龄66.9±9.7岁)的59处病变(8处闭塞;3处累及腘动脉段;病变长度:86.3±66.8mm)。
42处病变在BA前使用了旋磨术治疗,而17处病变首先通过BA进行再通。两组之间的临床和病变特征无差异。然而,旋磨术组中严重动脉夹层(C至F型)的发生率较低(88.2%对42.9%;P = 0.001)。多因素分析显示,使用旋磨术设备是预防严重夹层发生的唯一危险因素(P = 0.013;OR = 0.12;95%CI:0.025 - 0.642)。患者接受单纯血管成形术、药物涂层球囊或支架置入治疗。旋磨术组的靶血管再血管化和原发性通畅率呈较低趋势(秩和检验P = 0.108和0.166),然而继发性通畅率明显更好(秩和检验P = 0.001)。
BA前的旋磨术降低了严重夹层的发生率,因此可能是减少补救性支架置入需求的一个有价值的选择。