From the Division of Cardiology, Emory Clinical Cardiovascular Research Institute, Emory University School of Medicine (A.S.T., M.H., H.M.K., J.H.K., P.B.S., A.A., B.K., M.M.G., M.T., S.S.H., W.T.O., M.O., I.H., V.V., A.A.Q.).
Department of Biostatistics and Bioinformatics (Y.-A.K., C.L., E.M.).
Circ Res. 2018 Aug 3;123(4):467-476. doi: 10.1161/CIRCRESAHA.118.313282.
Blacks compared with whites have a greater risk of adverse cardiovascular outcomes. Impaired regenerative capacity, measured as lower levels of circulating progenitor cells (CPCs), is a novel determinant of adverse outcomes; however, little is known about racial differences in CPCs.
To investigate the number of CPCs, PC-mobilizing factors, PC mobilization during acute myocardial infarction and the predictive value of CPC counts in blacks compared with whites.
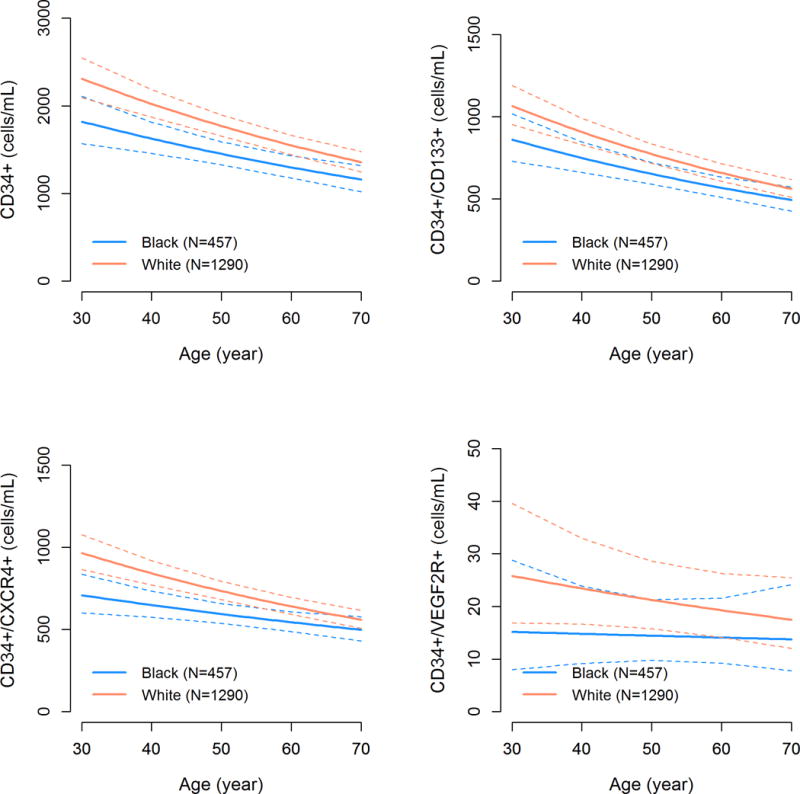
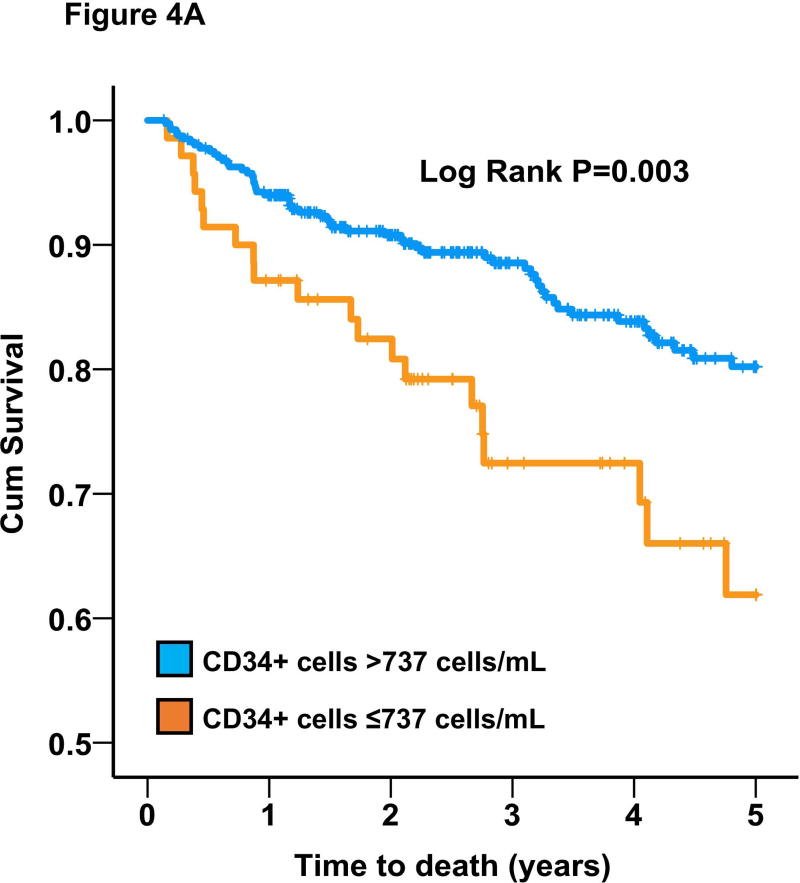
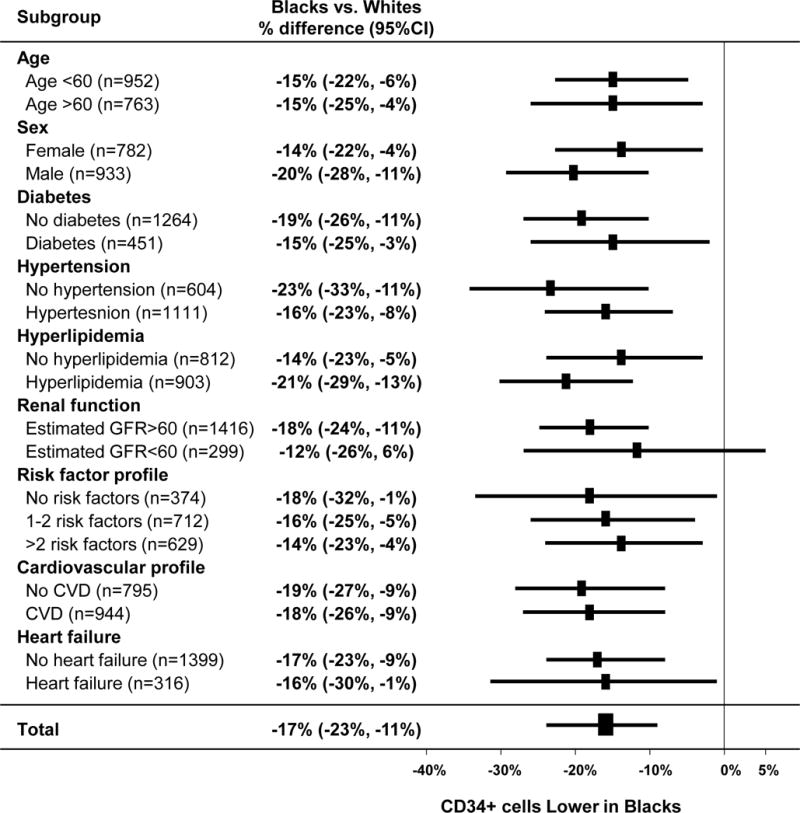
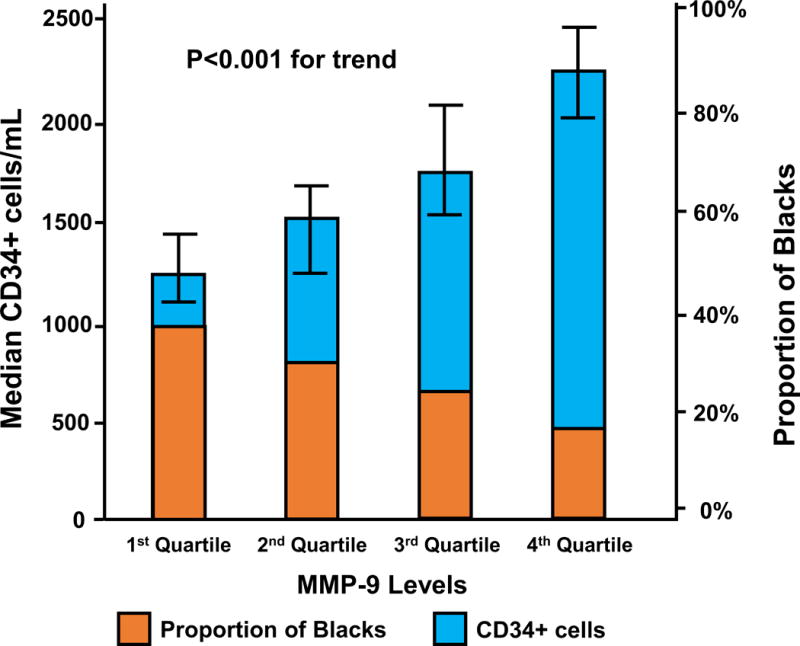
CPCs were enumerated by flow cytometry as CD45med blood mononuclear cells expressing CD34+, CD133+, VEGF2R+, and CXCR4+ epitopes in 1747 subjects, mean age 58.4±13, 55% male, and 26% self-reported black. Patients presenting with acute myocardial infarction (n=91) were analyzed separately. Models were adjusted for relevant clinical variables. SDF-1α (stromal cell-derived factor-1α), VEGF (vascular endothelial growth factor), and MMP-9 (matrix metallopeptidase-9) levels were measured (n=561), and 623 patients were followed for median of 2.2 years for survival analysis. Blacks were younger, more often female, with a higher burden of cardiovascular risk, and lower CPC counts. Blacks had fewer CD34+ cells (-17.6%; [95% confidence interval (CI), -23.5% to -11.3%]; P<0.001), CD34+/CD133+ cells (-15.5%; [95% CI, -22.4% to -8.1%]; P<0.001), CD34+/CXCR4+ cells (-17.3%; [95% CI, -23.9% to -10.2%]; P<0.001), and CD34+/VEGF2R+ cells (-27.9%; [95% CI, -46.9% to -2.0%]; P=0.04) compared with whites. The association between lower CPC counts and black race was not affected by risk factors or cardiovascular disease. Results were validated in a separate cohort of 411 patients. Blacks with acute myocardial infarction had significantly fewer CPCs compared with whites ( P=0.02). Blacks had significantly lower plasma MMP-9 levels ( P<0.001) which attenuated the association between low CD34+ and black race by 19% (95% CI, 13%-33%). However, VEGF and SDF-1α levels were not significantly different between the races. Lower CD34+ counts were similarly predictive of mortality in blacks (hazard ratio, 2.83; [95% CI, 1.12-7.20]; P=0.03) and whites (hazard ratio, 1.79; [95% CI, 1.09-2.94]; P=0.02) without significant interaction.
Black subjects have lower levels of CPCs compared with whites which is partially dependent on lower circulating MMP-9 levels. Impaired regenerative capacity is predictive of adverse outcomes in blacks and may partly account for their increased risk of cardiovascular events.
与白人相比,黑人发生不良心血管结局的风险更高。循环祖细胞(CPCs)水平较低表明再生能力受损,这是不良结局的一个新的决定因素;然而,关于 CPCs 的种族差异知之甚少。
研究黑人与白人相比,CPCs 的数量、PC 动员因子、急性心肌梗死期间的 PC 动员以及 CPC 计数的预测价值。
通过流式细胞术对 1747 例患者(平均年龄 58.4±13 岁,55%为男性,26%自我报告为黑人)的 CD45med 血液单核细胞中表达 CD34+、CD133+、VEGF2R+和 CXCR4+表型的 CPC 进行计数。分析了急性心肌梗死患者(n=91)的单独数据。对相关临床变量进行模型调整。测量了基质细胞衍生因子-1α(stromal cell-derived factor-1α,SDF-1α)、血管内皮生长因子(vascular endothelial growth factor,VEGF)和基质金属蛋白酶-9(matrix metallopeptidase-9,MMP-9)水平(n=561),并对 623 例患者进行了中位数为 2.2 年的生存分析。黑人更年轻,更多为女性,心血管风险负担更高,CPC 计数更低。黑人的 CD34+细胞数量减少(减少 17.6%;[95%置信区间(CI),-23.5%至-11.3%];P<0.001)、CD34+/CD133+细胞数量减少(减少 15.5%;[95% CI,-22.4%至-8.1%];P<0.001)、CD34+/CXCR4+细胞数量减少(减少 17.3%;[95% CI,-23.9%至-10.2%];P<0.001)、CD34+/VEGF2R+细胞数量减少(减少 27.9%;[95% CI,-46.9%至-2.0%];P=0.04)与白人相比。CPC 计数较低与黑人种族之间的关联不受危险因素或心血管疾病的影响。在另一个由 411 例患者组成的队列中验证了这些结果。与白人相比,急性心肌梗死的黑人患者的 CPC 明显减少(P=0.02)。黑人的 MMP-9 水平明显较低(P<0.001),这使 CD34+较低与黑人种族之间的关联降低了 19%(95%CI,13%-33%)。然而,VEGF 和 SDF-1α水平在不同种族之间没有明显差异。较低的 CD34+计数在黑人(危险比,2.83;[95%CI,1.12-7.20];P=0.03)和白人(危险比,1.79;[95%CI,1.09-2.94];P=0.02)中同样具有预测死亡的作用,且无显著交互作用。
与白人相比,黑人的 CPCs 水平较低,这部分归因于循环 MMP-9 水平较低。再生能力受损是黑人不良结局的预测因素,可能部分解释了他们心血管事件风险增加的原因。