First Department of Obstetrics and Gynecology, Semmelweis University, Baross str. 27, Budapest, H-1088, Hungary.
First Department of Pediatrics, Semmelweis University, Bókay János str. 53-54, Budapest, H-1083, Hungary.
J Neuroinflammation. 2018 Jun 22;15(1):191. doi: 10.1186/s12974-018-1229-y.
The perinatal period carries the highest risk for stroke in childhood; however, the pathophysiology is poorly understood and preventive, prognostic, and therapeutic strategies are not available. A new pathophysiological model describes the development of neonatal arterial ischemic stroke (NAIS) as the combined result of prenatal inflammation and hypoxic-ischemic insult. Neuroinflammation and a systemic inflammatory response are also important features of NAIS. Identifying key players of the inflammatory system is in the limelight of current research.
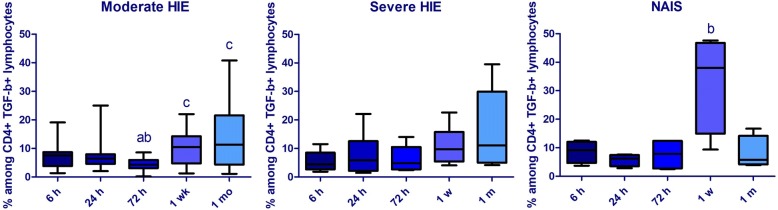
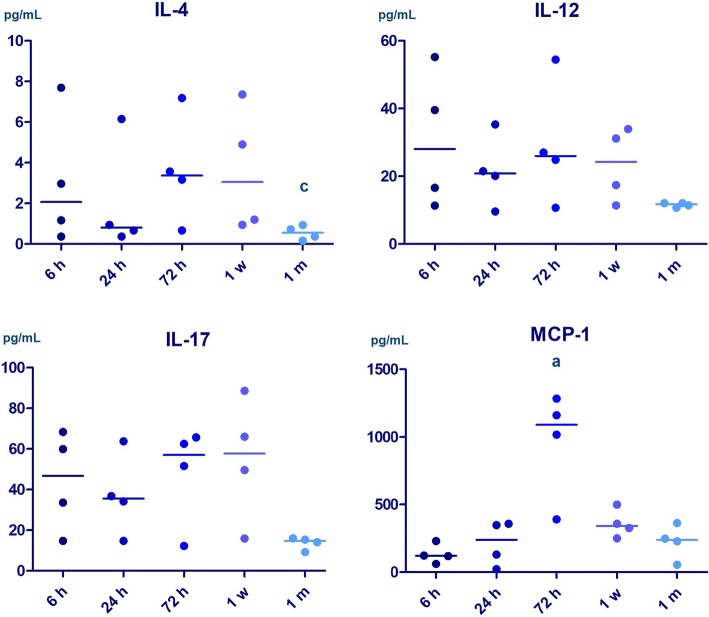
We present four NAIS cases, in whom detailed analysis of intracellular and plasma cytokine levels are available from the first month of life. All neonates were admitted with the initial diagnosis of hypoxic ischemic encephalopathy (HIE); however, early MRI examination revealed NAIS. Blood samples were collected between 3 and 6 h of life, at 24 h, 72 h, 1 week, and 1 month of life. Peripheral blood mononuclear cells were assessed with flow cytometry and plasma cytokine levels were measured. Pooled data from the cohort of four NAIS patients were compared to infants with HIE. At 6 and 72 h of age, the prevalence of IL10+ CD8+ lymphocytes remained lower in NAIS. At 6 h, CD8+ lymphocytes in NAIS produced more IL-17. At 72 h, CD8+ cells produced more IL-6 in severe HIE than in NAIS, but IL-6 production remained elevated in CD8 cells at 1 month in NAIS, while it decreased in HIE. At 1 week, the prevalence of TGF-β + lymphocytes prone to enter the CNS was elevated in NAIS. On the other hand, by 1 month of age, the prevalence of TGF-β + CD4+ lymphocytes decreased in NAIS compared to HIE. At 72 h, we found elevated plasma levels of IL-5, MCP-1, and IL-17 in NAIS. By 1 month, plasma levels of IL-4, IL-12, and IL-17 decreased in NAIS but remained elevated in HIE.
Differences in the cytokine network are present between NAIS and HIE. CD8 lymphocytes appear to shift towards the pro-inflammatory direction in NAIS. The inflammatory response appears to be more pronounced at 72 h in NAIS but decreases faster, reaching lower plasma levels of inflammatory markers at 1 month.
围产期是儿童中风风险最高的时期;然而,其病理生理学尚不清楚,也没有预防、预后和治疗策略。一个新的病理生理学模型将新生儿动脉缺血性中风(NAIS)的发展描述为产前炎症和缺氧缺血损伤的综合结果。神经炎症和全身炎症反应也是 NAIS 的重要特征。确定炎症系统的关键参与者是当前研究的焦点。
我们介绍了 4 例 NAIS 病例,其中从出生后的第一个月开始就可以对细胞内和血浆细胞因子水平进行详细分析。所有新生儿最初的诊断均为缺氧缺血性脑病(HIE);然而,早期 MRI 检查显示为 NAIS。在出生后 3-6 小时、24 小时、72 小时、1 周和 1 个月采集血样。用流式细胞术评估外周血单核细胞,测量血浆细胞因子水平。将 4 例 NAIS 患者的队列数据进行汇总,并与 HIE 患儿进行比较。在 6 和 72 小时时,IL10+CD8+淋巴细胞的患病率在 NAIS 中仍然较低。在 6 小时时,NAIS 中的 CD8+淋巴细胞产生更多的 IL-17。在 72 小时时,严重 HIE 中的 CD8+细胞产生的 IL-6 多于 NAIS,但在 NAIS 中,1 个月时 CD8 细胞中的 IL-6 产生仍保持升高,而在 HIE 中则降低。在 1 周时,NAIS 中倾向于进入中枢神经系统的 TGF-β+淋巴细胞的患病率升高。另一方面,在 1 个月时,与 HIE 相比,NAIS 中 TGF-β+CD4+淋巴细胞的患病率降低。在 72 小时时,我们发现 NAIS 中 IL-5、MCP-1 和 IL-17 的血浆水平升高。在 1 个月时,NAIS 中的 IL-4、IL-12 和 IL-17 的血浆水平降低,但在 HIE 中仍升高。
NAIS 和 HIE 之间存在细胞因子网络的差异。在 NAIS 中,CD8 淋巴细胞似乎向促炎方向转变。NAIS 中在 72 小时时炎症反应似乎更为明显,但下降较快,在 1 个月时达到较低的炎症标志物血浆水平。