School of Medicine, Stanford University, Stanford, CA, United States of America.
School of Medicine, University of California, San Francisco, CA, United States of America.
PLoS One. 2018 Jun 26;13(6):e0198912. doi: 10.1371/journal.pone.0198912. eCollection 2018.
Country decisions to scale-up "test and treat" approaches for HIV depend on consideration of both the health and economic consequences of such investments. Evidence about economic impacts of expanded antiretroviral therapy (ART) provision is particularly relevant for decisions regarding foreign assistance levels for HIV/AIDS programs. We used baseline data from the Sustainable East Africa Research in Community Health (SEARCH) cluster randomized controlled trial in Kenya and Uganda to examine the association between HIV status, CD4+ T-cell counts, viral suppression, and multiple indicators of economic well-being.
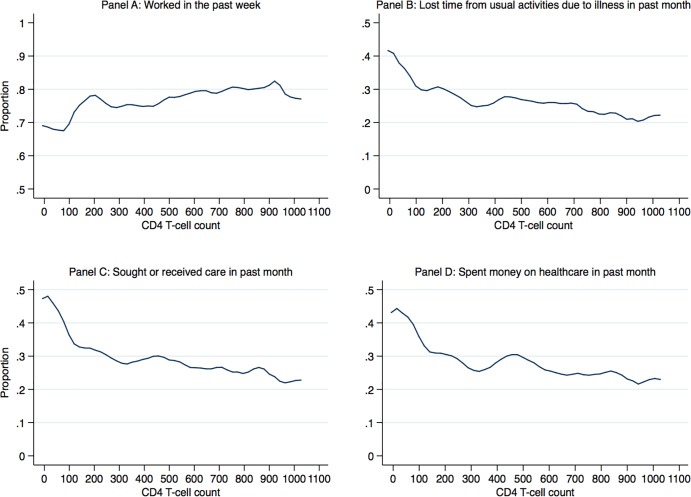
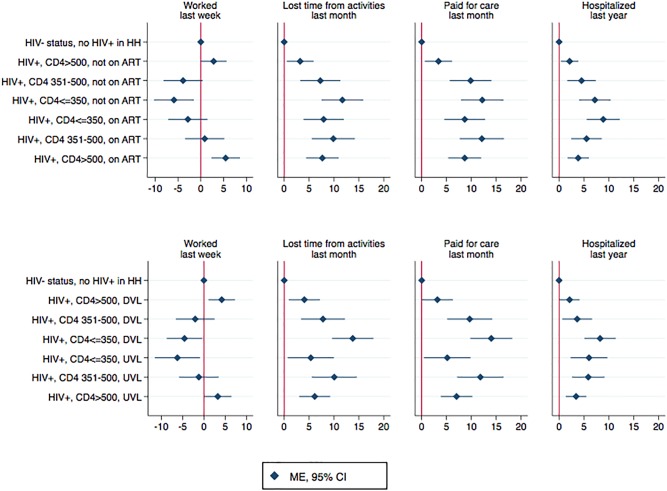
Socio-economic surveys were conducted in households with HIV-positive and HIV-negative adults sampled after a census of 32 communities participating in the SEARCH trial (NCT01864603). Data were obtained for 11,500 individuals from 5,884 households in study communities. Participants were stratified based on their own HIV status as well as CD4 counts and viral suppression status if they were HIV-positive. HIV-negative participants residing in households with no HIV-positive adults were considered separately from HIV-negative participants residing in households with ≥1 HIV-positive adult. Generalized estimating equation models were used to examine the relationship between HIV status, CD4 counts, ART, viral suppression, and outcomes of employment, self-reported illness, lost time from usual activities due to illness, healthcare utilization, health expenditures, and hospitalizations. In all models, HIV-negative participants in households with no HIV-positive persons were the reference group. There was no significant difference in the probability of being employed between HIV-positive participants with CD4>500 and the reference group of HIV-negative participants residing in households with no HIV-positive adults (marginal effect, ME, 1.49 percentage points; 95% confidence interval, CI, -1.09, 4.08). However, HIV-positive participants with CD4 351-500 were less likely to be employed than the reference group (ME -4.50, 95% CI -7.99, -1.01), as were HIV-positive participants with CD4 ≤350 (ME -7.41, 95% CI -10.96, -3.85). Similarly, there was no significant difference in employment likelihood between HIV-negative participants who resided in households with a CD4>500 HIV-positive person and the reference group (ME -1.78, 95% CI -5.16, 1.59). HIV-negative participants residing with an HIV-positive person with CD4 351-500, however, were less likely to be employed than the reference group (ME -7.03, 95% CI -11.49, -2.57), as were people residing with a household member with CD4 ≤350 (ME -6.28, 95% CI -10.76, -1.80). HIV-positive participants in all CD4 categories were more likely to have lost time from usual activities due to illness and have incurred healthcare expenditures. Those with CD4>500 had better economic outcomes than those with CD4 351-500, even among those not virally suppressed (p = 0.004) and not on ART (p = 0.01).
Data from a large population-representative sample of households in east Africa showed a strong association between the health of HIV-positive persons and economic outcomes. The findings suggest there may be economic benefits associated with maintaining high CD4 counts, both for HIV-positive persons and their HIV-negative household members. The association of high CD4 counts with improved outcomes is consistent with the hypothesis that early ART initiation can avert declines in employment and other economic outcomes. Prospective longitudinal evaluation is needed to assess the causal impact of early ART initiation on economic functioning of households.
国家是否扩大“检测和治疗”艾滋病的措施取决于对这些投资的健康和经济后果的考虑。关于扩大抗逆转录病毒疗法(ART)提供的经济影响的证据对于有关艾滋病毒/艾滋病方案外国援助水平的决策特别重要。我们使用肯尼亚和乌干达的东非可持续社区健康研究(SEARCH)集群随机对照试验的基线数据,研究了艾滋病毒状况、CD4+T 细胞计数、病毒抑制与多种经济福祉指标之间的关联。
在参与 SEARCH 试验的 32 个社区进行了人口普查后,对艾滋病毒阳性和艾滋病毒阴性成年人的家庭进行了社会经济调查(NCT01864603)。从研究社区的 5884 户家庭中获得了 11500 名个人的数据。参与者根据自身的艾滋病毒状况以及 CD4 计数和病毒抑制状况进行分层,如果他们是艾滋病毒阳性,则根据 CD4 计数和病毒抑制状况进行分层。没有艾滋病毒阳性成年人的家庭中的艾滋病毒阴性参与者与至少有 1 名艾滋病毒阳性成年人的家庭中的艾滋病毒阴性参与者分开考虑。使用广义估计方程模型来检查艾滋病毒状况、CD4 计数、ART、病毒抑制与就业、自我报告疾病、因疾病而缺勤、医疗保健利用、卫生支出和住院的结果之间的关系。在所有模型中,没有艾滋病毒阳性者的家庭中的艾滋病毒阴性参与者是参照组。CD4>500 的艾滋病毒阳性参与者与没有艾滋病毒阳性成年人的家庭中的艾滋病毒阴性参照组参与者的就业概率没有显著差异(边际效应,ME,1.49 个百分点;95%置信区间,CI,-1.09,4.08)。然而,CD4 351-500 的艾滋病毒阳性参与者的就业可能性低于参照组(ME-4.50,95%CI-7.99,-1.01),CD4≤350 的艾滋病毒阳性参与者也是如此(ME-7.41,95%CI-10.96,-3.85)。同样,CD4>500 的艾滋病毒阳性者家庭中的艾滋病毒阴性参与者与参照组之间的就业可能性没有显著差异(ME-1.78,95%CI-5.16,1.59)。然而,与参照组相比,与 CD4 351-500 的艾滋病毒阳性者同住的艾滋病毒阴性参与者更不可能就业(ME-7.03,95%CI-11.49,-2.57),与与 CD4≤350 的家庭成员同住的人也是如此(ME-6.28,95%CI-10.76,-1.80)。所有 CD4 类别中的艾滋病毒阳性者因疾病缺勤和产生医疗保健支出的可能性更高。那些 CD4>500 的人即使在没有病毒抑制(p=0.004)和没有接受 ART(p=0.01)的情况下,也比 CD4 351-500 的人有更好的经济结果。
来自东非大型代表性家庭样本的数据显示,艾滋病毒阳性者的健康状况与经济结果之间存在很强的关联。这些发现表明,保持较高的 CD4 计数可能会带来经济上的好处,无论是对艾滋病毒阳性者还是他们的艾滋病毒阴性家庭成员都是如此。高 CD4 计数与改善结果之间的关联与早期 ART 启动可以避免就业和其他经济结果下降的假设是一致的。需要进行前瞻性纵向评估,以评估早期 ART 启动对家庭经济功能的因果影响。