Division of Gastroenterology, Massachusetts General Hospital, Boston, Massachusetts.
Division of Gastroenterology, Johns Hopkins Hospital, Baltimore, Maryland.
Clin Gastroenterol Hepatol. 2019 Feb;17(3):502-509.e1. doi: 10.1016/j.cgh.2018.06.031. Epub 2018 Jun 23.
BACKGROUND & AIMS: In patients with acute severe ulcerative colitis (ASUC), standard infliximab induction therapy has modest efficacy. There are limited data on the short-term or long-term efficacy of accelerated infliximab induction therapy for these patients.
In a retrospective study, we collected data from 213 patients with steroid refractory ASUC who received infliximab rescue therapy at 3 centers, from 2005 through 2017. Patients were classified that received standard therapy (5mg/kg infliximab at weeks 0, 2, and 6) or accelerated therapy (>5mg/kg infliximab at shorter intervals). The primary outcome was colectomy in-hospital and at 3, 6, 12, and 24 months. Multivariable regression models were adjusted for relevant confounders. We also performed a meta-analysis of published effects of standard vs accelerated infliximab treatment of ASUC.
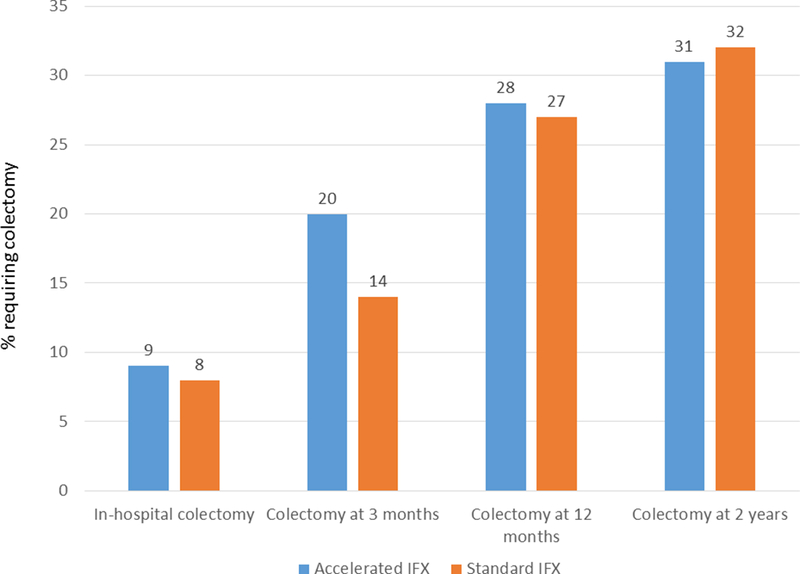
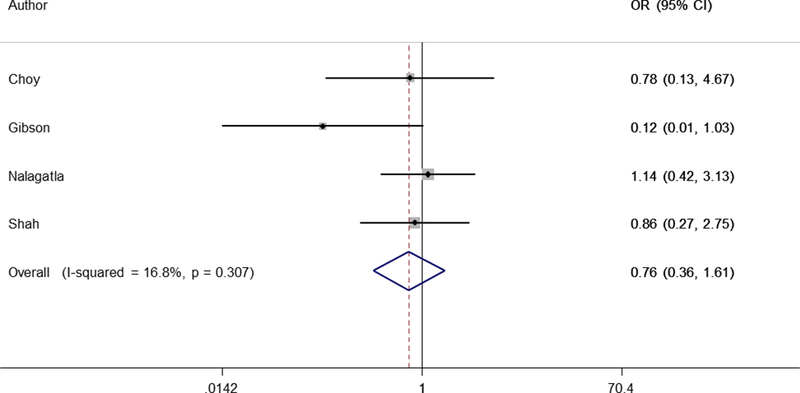
In the retrospective analysis, 81 patients received accelerated infliximab therapy and 132 received standard infliximab therapy. There were no differences in characteristics between the groups, including levels of C-reactive protein or albumin. Similar proportions of patients in each group underwent in-hospital colectomy (9% receiving accelerated therapy vs 8% receiving standard therapy; adjusted odds ratio, 1.35; 95% CI, 0.38-4.82). There was no significant difference between groups in proportions that underwent colectomy at 3, 6, 12, or 24 months (P > .20 for all comparisons). Among those in the accelerated group, an initial dose of 10 mg/kg was associated with a lower rate of colectomy compared to patients who initially received 5 mg/kg followed by subsequent doses of 5mg/kg or higher. Our systematic review identified 7 studies (181 patients receiving accelerated infliximab and 436 receiving standard infliximab) and found no significant differences in short- or long-term outcomes.
In a retrospective study and meta-analysis, we found no association between accelerated infliximab induction therapy and lower rates of colectomy in patients with ASUC, compared to standard induction therapy. However, confounding by disease severity cannot be excluded. Randomized trials are warranted to compare these treatment strategies.
在急性重度溃疡性结肠炎(ASUC)患者中,标准英夫利昔单抗诱导治疗的疗效有限。关于这些患者接受加速英夫利昔单抗诱导治疗的短期或长期疗效的数据有限。
在一项回顾性研究中,我们从 2005 年至 2017 年,从 3 个中心收集了 213 例接受英夫利昔单抗解救治疗的类固醇难治性 ASUC 患者的数据。患者分为接受标准治疗(第 0、2 和 6 周时给予 5mg/kg 英夫利昔单抗)或加速治疗(更短时间间隔给予>5mg/kg 英夫利昔单抗)。主要结局是住院和 3、6、12 和 24 个月时的结肠切除术。多变量回归模型调整了相关混杂因素。我们还对标准与加速英夫利昔单抗治疗 ASUC 的效果进行了荟萃分析。
在回顾性分析中,81 例患者接受加速英夫利昔单抗治疗,132 例患者接受标准英夫利昔单抗治疗。两组患者的特征无差异,包括 C 反应蛋白或白蛋白水平。每组均有相似比例的患者接受住院结肠切除术(接受加速治疗的患者为 9%,接受标准治疗的患者为 8%;调整后的优势比,1.35;95%CI,0.38-4.82)。两组在 3、6、12 或 24 个月时进行结肠切除术的比例无显著差异(所有比较 P>.20)。在加速组中,与初始给予 5mg/kg 然后给予更高剂量的患者相比,初始给予 10mg/kg 的患者结肠切除术的发生率较低。我们的系统评价确定了 7 项研究(181 例接受加速英夫利昔单抗治疗和 436 例接受标准英夫利昔单抗治疗),发现短期和长期结局均无显著差异。
在回顾性研究和荟萃分析中,与标准诱导治疗相比,我们发现加速英夫利昔单抗诱导治疗与 ASUC 患者较低的结肠切除术率之间没有关联。然而,不能排除疾病严重程度的混杂因素。需要进行随机试验来比较这些治疗策略。