Cardiovascular Center, Seoul National University Bundang Hospital, Seongnam, Korea.
Korean J Intern Med. 2019 Jul;34(4):819-829. doi: 10.3904/kjim.2017.378. Epub 2018 Jul 4.
BACKGROUND/AIMS: After a study comparing drug-eluting stents (DESs) to sequential treatment with drug-eluting balloons (DEBs) and bare metal stents (BMSs), we retrospectively analysed strut malapposition and neointimal hyperplasia in de novo coronary lesions using optical coherence tomography (OCT) or intravascular ultrasonography (IVUS).
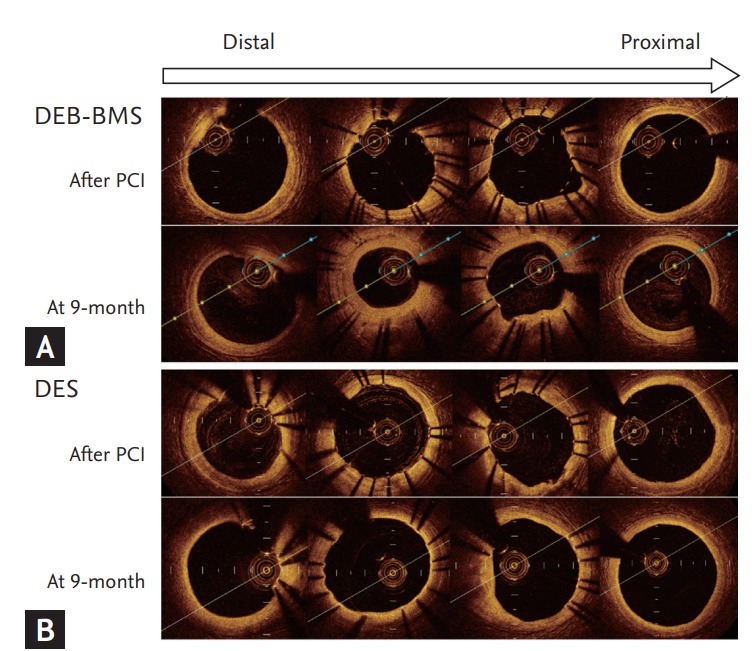
We obtained OCT data from 16 patients (eight per group) and IVUS data from 40 patients (20 per group). OCT or IVUS was performed after the index procedure and after 9 months. Parameters including obstruction volume due to neointimal hyperplasia (neointimal hyperplasia volume/stent volume, %), strut malapposition (% of malapposed struts), and intra-individual inhomogeneity of in-stent restenosis were compared.
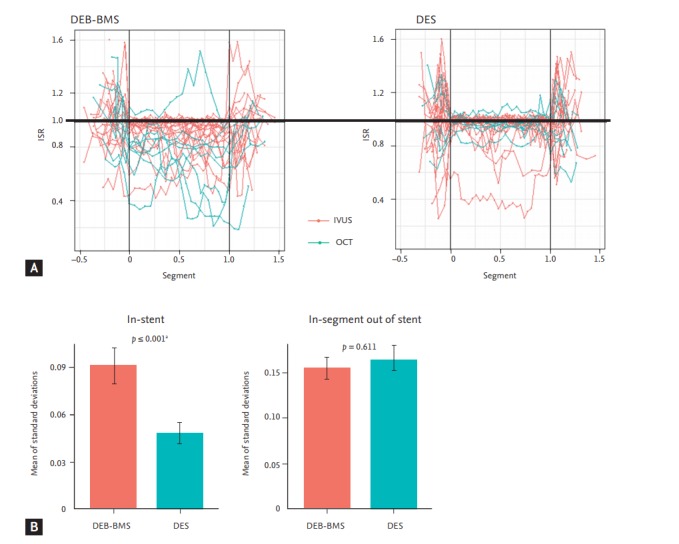
Although obstruction volume due to neointimal hyperplasia was significantly higher in the DEB-BMS group (14.90 ± 15.36 vs. DES 7.03 ± 11.39, p = 0.025), there was no difference in strut malapposition between the two groups (DEB-BMS 1.99 ± 5.37 vs. DES 0.88 ± 2.22, p = 0.856). The DEB-BMS group showed greater intra-individual inhomogeneity of in-stent restenosis pattern than the DES group.
Treatment with DEB followed by BMS failed to improve strut malapposition despite higher in-stent neointimal growth, probably because of the inhomogeneous inhibition of in-stent neointimal hyperplasia by DEB. DEB technology should be improved to obtain even drug delivery to the vessel wall and homogeneous prevention of neointimal growth comparable to contemporary DES.
背景/目的:在一项比较药物洗脱支架(DES)与药物洗脱球囊(DEB)序贯治疗和裸金属支架(BMS)的研究之后,我们使用光学相干断层扫描(OCT)或血管内超声(IVUS)对新发冠状动脉病变中的支架贴壁不良和新生内膜增生进行了回顾性分析。
我们从 16 名患者(每组 8 名)中获得了 OCT 数据,从 40 名患者(每组 20 名)中获得了 IVUS 数据。在指数操作后和 9 个月后进行 OCT 或 IVUS。比较了包括新生内膜增生导致的阻塞体积(新生内膜增生体积/支架体积,%)、支架贴壁不良(贴壁不良支架的%)和支架内再狭窄的个体内异质性等参数。
尽管 DEB-BMS 组的新生内膜增生导致的阻塞体积显著更高(14.90±15.36 比 DES 组 7.03±11.39,p=0.025),但两组之间的支架贴壁不良没有差异(DEB-BMS 组 1.99±5.37 比 DES 组 0.88±2.22,p=0.856)。DEB-BMS 组的支架内再狭窄模式个体内异质性大于 DES 组。
尽管支架内新生内膜增生更高,但 DEB 联合 BMS 治疗未能改善支架贴壁不良,可能是由于 DEB 对支架内新生内膜增生的不均匀抑制。DEB 技术应加以改进,以实现对血管壁的均匀药物输送和与当代 DES 相当的均匀新生内膜增生预防。