Jin Min Ji, Kim Yunkyum, Choi Eun Mi, Shim Ye Jee, Kim Heung Sik, Suh Jin Kyung, Kim Ji Yoon, Lee Kun Soo, Park Sun Young, Lee Jae Min, Hah Jeong Ok
Department of Pediatrics, Keimyung University School of Medicine and Dongsan Medical Center, Daegu, Korea.
Department of Pediatrics, Gachon University Gil Medical Center, Incheon, Korea.
Blood Res. 2018 Jun;53(2):110-116. doi: 10.5045/br.2018.53.2.110. Epub 2018 Jun 25.
Cytomegalovirus (CMV) causes severe diseases in premature infants and immunocompromised hosts, and antiviral therapy is often required for disease control. However, the clinical manifestations and treatment courses for CMV-associated thrombocytopenia in immunocompetent children are unclear.
Medical records of the children who suffered from thrombocytopenia, and showed positive CMV polymerase chain reaction and CMV-like symptoms were retrospectively analyzed at three university hospitals in Daegu from January 2000 to March 2017. Patients suffering from leukemia, immunodeficiency, and other infections were excluded.
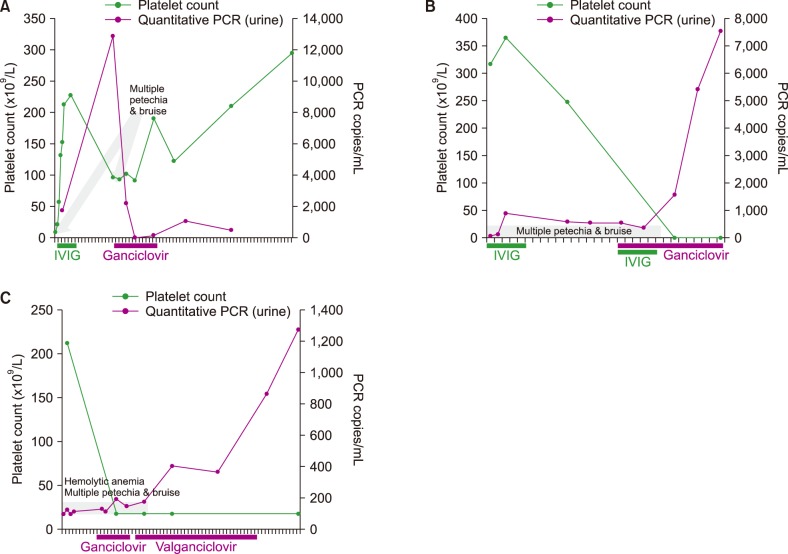
Among 1,065 children with thrombocytopenia, 29 (2.7%) displayed CMV-associated thrombocytopenia. The median age at diagnosis was 15 months and the median platelet count was 26,000/µL. They were classified into the CMV-induced thrombocytopenia (23/29) and CMV-related secondary immune thrombocytopenia (ITP, 6/29) groups. Fourteen subjects had hepatic dysfunction, four had Evans syndrome, two had pneumonitis, and one had gastritis. IVIG was used for 21 patients, and six patients among them showed recurrence, for whom IVIG or antiviral therapy was used. All, except one, recurrent or chronic cases belonged to the CMV-induced thrombocytopenia group. Antiviral therapy was used more frequently for the CMV-induced thrombocytopenia group (8/23, 34.8%) than for the CMV-related secondary ITP group (0/6); however, the results were not statistically significant (=0.148).
CMV is a rare but unique etiology of thrombocytopenia, and observed even in healthy children after the neonatal period. About one-third patients need antiviral therapy for disease control. Further, CMV-induced thrombocytopenia is more complex than CMV-related secondary ITP.
巨细胞病毒(CMV)可导致早产儿和免疫功能低下宿主发生严重疾病,通常需要抗病毒治疗来控制病情。然而,免疫功能正常儿童中CMV相关性血小板减少症的临床表现和治疗过程尚不清楚。
回顾性分析2000年1月至2017年3月大邱市三家大学医院收治的血小板减少且CMV聚合酶链反应呈阳性并伴有CMV样症状的儿童病历。排除患有白血病、免疫缺陷和其他感染的患者。
在1065例血小板减少症患儿中,29例(2.7%)表现为CMV相关性血小板减少症。诊断时的中位年龄为15个月,中位血小板计数为26,000/µL。他们被分为CMV诱导的血小板减少症组(23/29)和CMV相关的继发性免疫性血小板减少症(ITP,6/29)组。14例患者有肝功能障碍,4例有伊文氏综合征,2例有肺炎,1例有胃炎。21例患者使用了静脉注射免疫球蛋白(IVIG),其中6例复发,对这6例复发患者再次使用了IVIG或抗病毒治疗。除1例患者外,所有复发或慢性病例均属于CMV诱导的血小板减少症组。CMV诱导的血小板减少症组(8/23,34.8%)比CMV相关的继发性ITP组(0/6)更频繁地使用抗病毒治疗;然而,结果无统计学意义(P=0.148)。
CMV是血小板减少症的一种罕见但独特的病因,甚至在新生儿期后的健康儿童中也有观察到。约三分之一的患者需要抗病毒治疗来控制病情。此外,CMV诱导的血小板减少症比CMV相关的继发性ITP更复杂。