Ozkaynak M Fevzi, Gilman Andrew L, London Wendy B, Naranjo Arlene, Diccianni Mitchell B, Tenney Sheena C, Smith Malcolm, Messer Karen S, Seeger Robert, Reynolds C Patrick, Smith L Mary, Shulkin Barry L, Parisi Marguerite, Maris John M, Park Julie R, Sondel Paul M, Yu Alice L
New York Medical College, Valhalla, NY, United States.
Levine Children's Hospital, Charlotte, NC, United States.
Front Immunol. 2018 Jun 18;9:1355. doi: 10.3389/fimmu.2018.01355. eCollection 2018.
A phase 3 randomized study (COG ANBL0032) demonstrated significantly improved outcome by adding immunotherapy with ch14.18 antibody to isotretinoin as post-consolidation therapy for high-risk neuroblastoma (NB). This study, ANBL0931, was designed to collect FDA-required safety/toxicity data to support FDA registration of ch14.18.
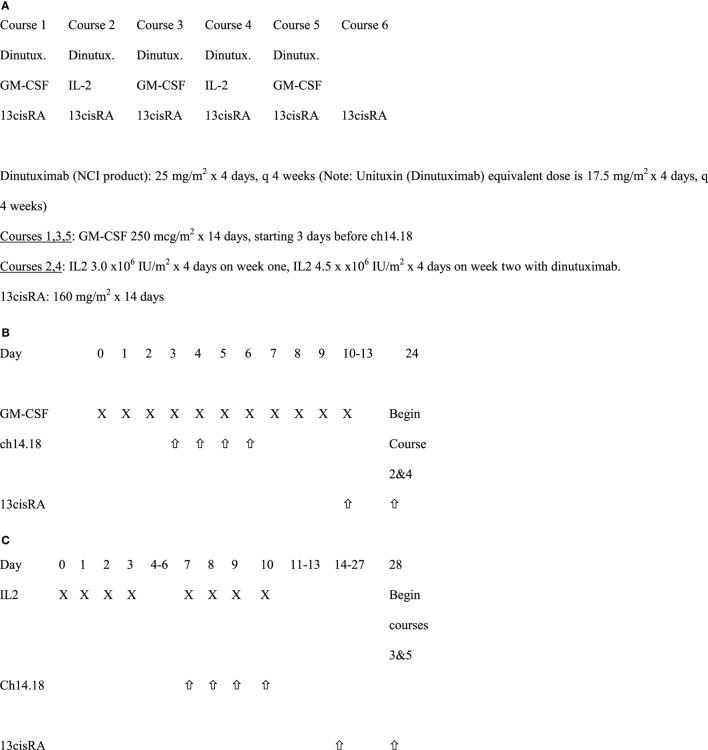
Newly diagnosed high-risk NB patients who achieved at least a partial response to induction therapy and received myeloablative consolidation with stem cell rescue were enrolled to receive six courses of isotretinoin with five concomitant cycles of ch14.18 combined with GM-CSF or IL2. Ch14.18 infusion time was 10-20 h per dose. Blood was collected for cytokine analysis and its association with toxicities and outcome.
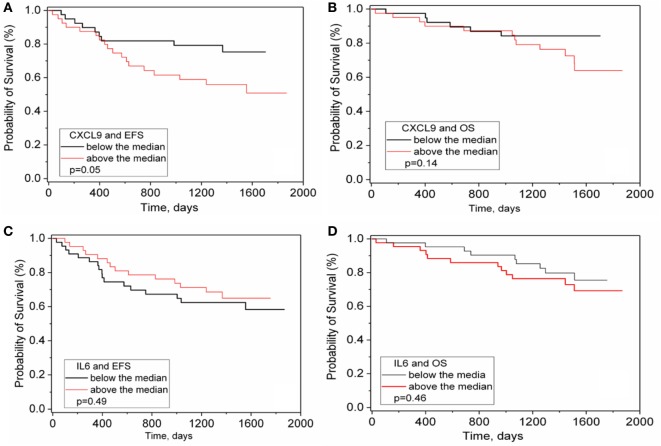
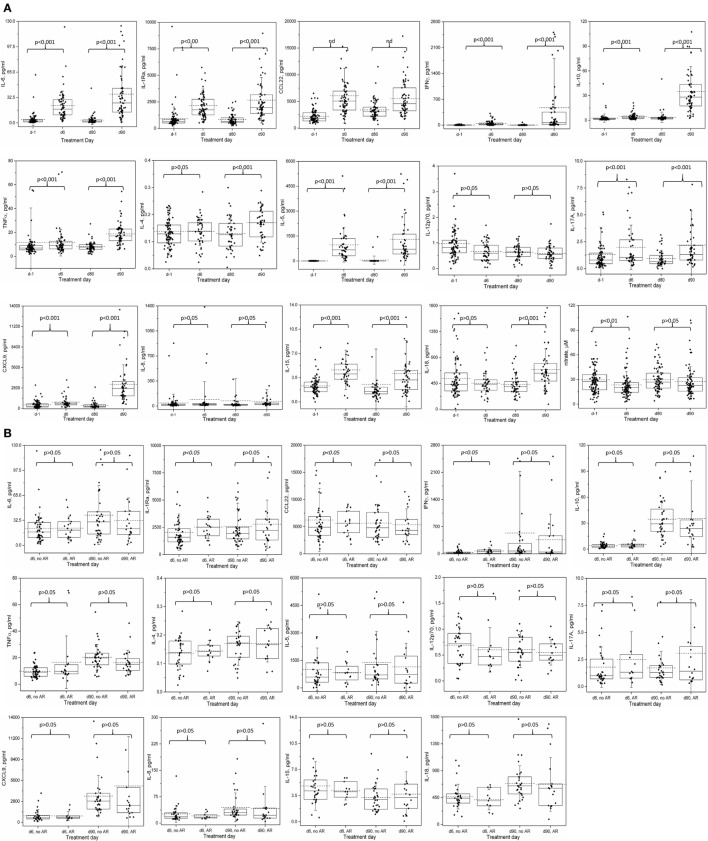
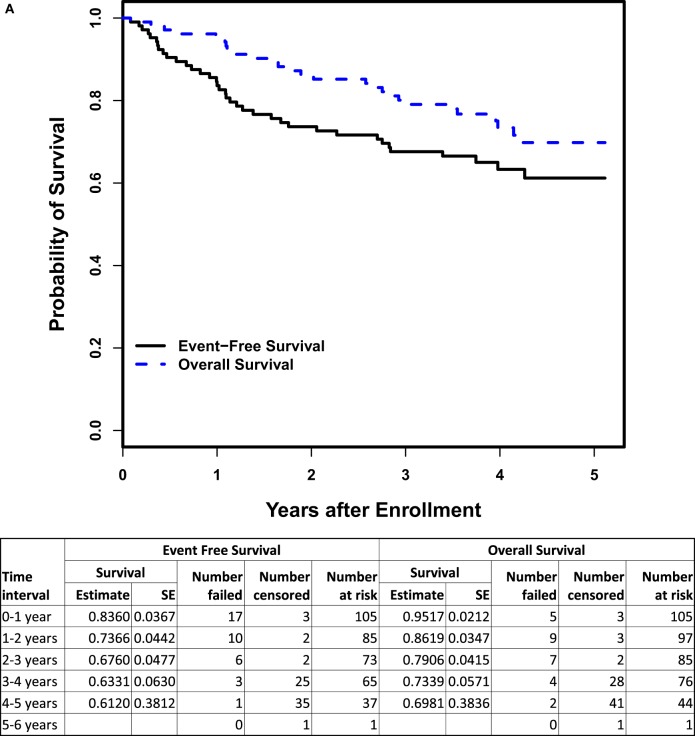
Of 105 patients enrolled, five patients developed protocol-defined unacceptable toxicities. The most common grade ≥ 3 non-hematologic toxicities of immunotherapy for cycles 1-5, respectively, were neuropathic pain (41, 28, 22, 31, 24%), hypotension (10, 17, 4, 14, 8%), allergic reactions (ARs) (3, 10, 5, 7, 2%), capillary leak syndrome (1, 4, 0, 2, 0%), and fever (21, 59, 6, 32, 5%). The 3-year event-free survival and overall survival were 67.6 ± 4.8% and 79.1 ± 4.2%, respectively. AR during course 1 was associated with elevated serum levels of IL-1Ra and IFNγ, while severe hypotension during this course was associated with low IL5 and nitrate. Higher pretreatment CXCL9 level was associated with poorer event-free survival (EFS).
This study has confirmed the significant, but manageable treatment-related toxicities of this immunotherapy and identified possible cytokine biomarkers associated with select toxicities and outcome. EFS and OS appear similar to that previously reported on ANBL0032.
一项3期随机研究(COG ANBL0032)表明,对于高危神经母细胞瘤(NB),在异维A酸巩固治疗后添加ch14.18抗体免疫疗法可显著改善预后。本研究ANBL0931旨在收集美国食品药品监督管理局(FDA)要求的安全性/毒性数据,以支持ch14.18的FDA注册。
新诊断的高危NB患者,对诱导治疗至少有部分反应且接受了清髓性巩固治疗并进行了干细胞救援,入组接受六个疗程的异维A酸治疗,同时进行五个周期的ch14.18联合粒细胞巨噬细胞集落刺激因子(GM-CSF)或白细胞介素2(IL2)治疗。每次ch14.18输注时间为每剂10 - 20小时。采集血液进行细胞因子分析及其与毒性和预后的关联研究。
105例入组患者中,5例出现方案定义的不可接受毒性。第1 - 5周期免疫疗法最常见的≥3级非血液学毒性分别为神经性疼痛(41%、28%、22%、31%、24%)、低血压(10%、17%、4%、14%、8%)、过敏反应(ARs)(3%、10%、5%、7%、2%)、毛细血管渗漏综合征(1%、4%、0%、2%、0%)和发热(21%、59%、6%、32%、5%)。3年无事件生存率和总生存率分别为67.6±4.8%和79.1±4.2%。第1疗程的AR与血清白细胞介素-1受体拮抗剂(IL-1Ra)和干扰素γ(IFNγ)水平升高相关,而该疗程的严重低血压与低IL5和硝酸盐相关。治疗前较高的CXC趋化因子配体9(CXCL9)水平与较差的无事件生存率(EFS)相关。
本研究证实了这种免疫疗法具有显著但可控的治疗相关毒性,并确定了与特定毒性和预后相关的可能细胞因子生物标志物。EFS和总生存期(OS)似乎与之前ANBL0032报道的相似。