Department of Dermatology, Centre Hospitalier Lyon Sud, Hospices Civils de Lyon, Lyon 1 University, 165 Chemin du Grand Revoyet, 69495, Pierre Bénite Cedex, France.
Unit of Epidemiology and Infection Control Unit, Hôpital Edouard Herriot, Hospices Civils de Lyon, Laboratory of Emergent Pathogens, CIRI, Claude Bernard Lyon 1 University, Lyon, France.
BMC Cancer. 2018 Jul 3;18(1):705. doi: 10.1186/s12885-018-4618-9.
Anti-PD-1 and BRAF-inhibitors (BRAFi) have been approved as first-line treatments in advanced melanoma. To date, no prospective data are available to give the best sequence of treatment. The objective of this study was to evaluate in real-life the efficacy of anti-PD-1 after BRAFi, ipilimumab, or chemotherapy failure.
This was a single institution cohort analysis in patients treated with anti-PD-1 right after BRAFi, ipilimumab, or chemotherapy failure. Melanoma evolution after anti-PD-1 initiation was analyzed in BRAF-mutated and BRAF wild-type patients. The efficacy of treatment was evaluated by Objective Response Rate (ORR), Disease Control Rate (DCR), Progression-Free Survival (PFS), and Overall Survival (OS).
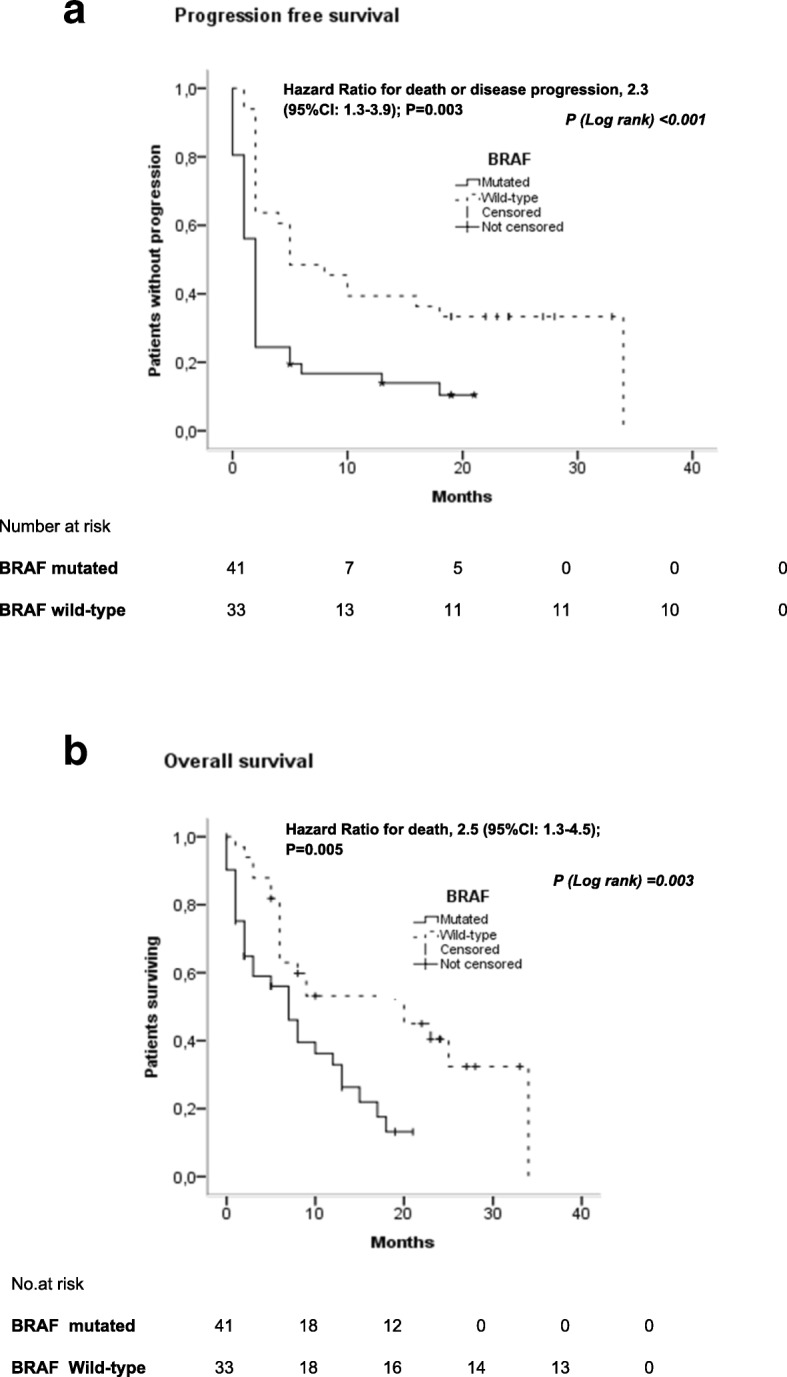
Seventy-four patients were included: 33 wild-type and 41 BRAF-mutated melanoma. ORR to anti-PD-1 was significantly lower in BRAF-mutated patients (12.2% vs. 45.5%, p = 0.002). After anti-PD-1 initiation, the median PFS and OS was significantly shorter in the BRAF mutated group (2 vs. 5 months and 7 vs. 20 months, p = 0.001). The hazard ratio for disease progression was of 2.3 (95%CI:1.3-3.9; p = 0.003) and 2.5 (95%CI:1.3-4.5; p = 0.005) for death. Thirty-nine percent of BRAF-mutated-patients died within 3 months after anti-PD-1 initiation. Rapid death (≤3 months) was significantly higher in BRAF-mutated patients (55.2% vs. 20.0%, p = 0.014).
This is the largest series of unselected patients treated in real-life with anti-PD-1 as second-or-higher line of treatment. Anti-PD-1 was less effective in BRAF-mutated cases as a majority of patients presented aggressive tumor evolution after BRAFi discontinuation. These data are consistent with previous studies suggesting a negative impact of BRAFi prior to immunotherapy.
抗 PD-1 和 BRAF 抑制剂(BRAFi)已被批准作为晚期黑色素瘤的一线治疗方法。迄今为止,尚无前瞻性数据可以提供最佳的治疗顺序。本研究的目的是在真实环境中评估抗 PD-1 在 BRAFi、伊匹单抗或化疗失败后的疗效。
这是一项单机构队列分析,纳入了在 BRAFi、伊匹单抗或化疗失败后立即接受抗 PD-1 治疗的患者。分析了抗 PD-1 治疗开始后 BRAF 突变和 BRAF 野生型患者的黑色素瘤进展情况。通过客观缓解率(ORR)、疾病控制率(DCR)、无进展生存期(PFS)和总生存期(OS)评估治疗效果。
共纳入 74 例患者:33 例为 BRAF 野生型,41 例为 BRAF 突变型黑色素瘤。BRAF 突变型患者的抗 PD-1 客观缓解率明显较低(12.2% vs. 45.5%,p=0.002)。抗 PD-1 治疗开始后,BRAF 突变组的中位 PFS 和 OS 明显缩短(2 个月 vs. 5 个月和 7 个月 vs. 20 个月,p=0.001)。疾病进展的风险比为 2.3(95%CI:1.3-3.9;p=0.003)和 2.5(95%CI:1.3-4.5;p=0.005),死亡风险比为 2.3(95%CI:1.3-3.9;p=0.003)和 2.5(95%CI:1.3-4.5;p=0.005)。抗 PD-1 治疗开始后 3 个月内,39%的 BRAF 突变型患者死亡。BRAF 突变型患者快速死亡(≤3 个月)明显较高(55.2% vs. 20.0%,p=0.014)。
这是最大的一系列未经选择的患者在真实环境中接受抗 PD-1 作为二线或更高线治疗的系列研究。抗 PD-1 在 BRAF 突变型病例中的疗效较低,因为大多数患者在 BRAFi 停药后表现出侵袭性肿瘤进展。这些数据与先前的研究一致,表明 BRAFi 在前免疫治疗时具有负面影响。