Department of Anesthesiology and Critical Care Medicine, Children's Hospital of Philadelphia and University of Pennsylvania, 6040A Wood Building, 34th Street and 3401 Civic Center Boulevard, Philadelphia, PA, 19104, USA.
Division of Pediatric Critical Care Medicine, Department of Pediatrics and Public Health Science, Penn State Hershey Children's Hospital, 500 University Drive, Hershey, PA, 17033, USA.
Intensive Care Med. 2018 Aug;44(8):1230-1239. doi: 10.1007/s00134-018-5286-6. Epub 2018 Jul 3.
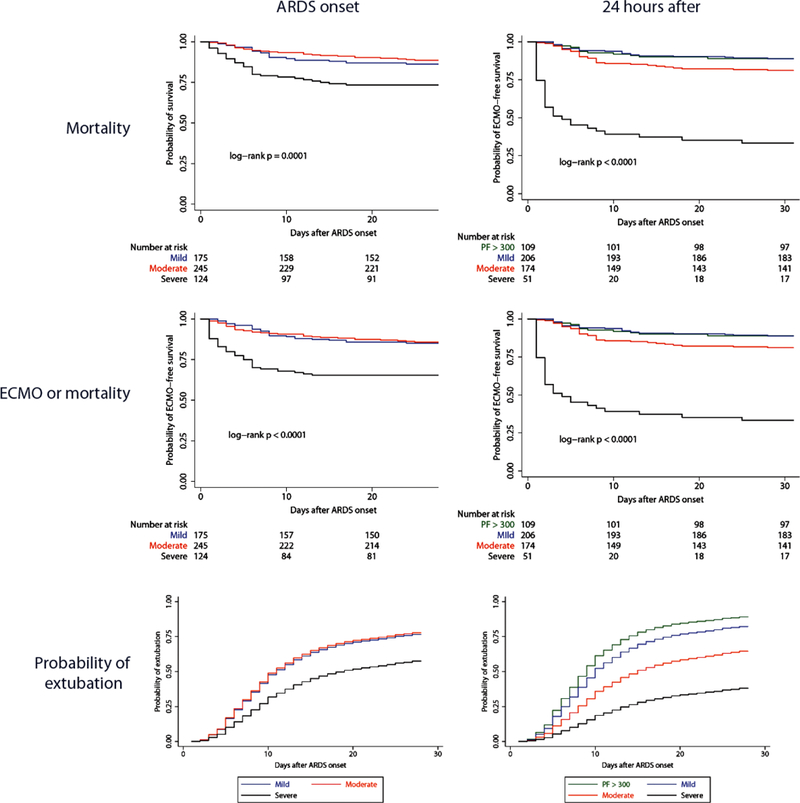
Acute respiratory distress syndrome (ARDS) is heterogeneous in etiology, which may affect outcomes. Stratification into biologically-defined subtypes may reduce heterogeneity. However, it is unknown whether pediatric ARDS has clinically relevant subtypes. We aimed to determine whether clinical characteristics and predictors of mortality differed between direct and indirect ARDS, and separately between infectious and non-infectious ARDS.
This was a single center, prospective cohort study of 544 children with ARDS (Berlin) between July 2011 and June 2017, stratified into direct versus indirect ARDS, and separately into infectious versus non-infectious ARDS. Multiple logistic regression was used to test for predictors of mortality in the entire cohort, and separately within subtypes. Effect modification by subtype was assessed using interaction tests.
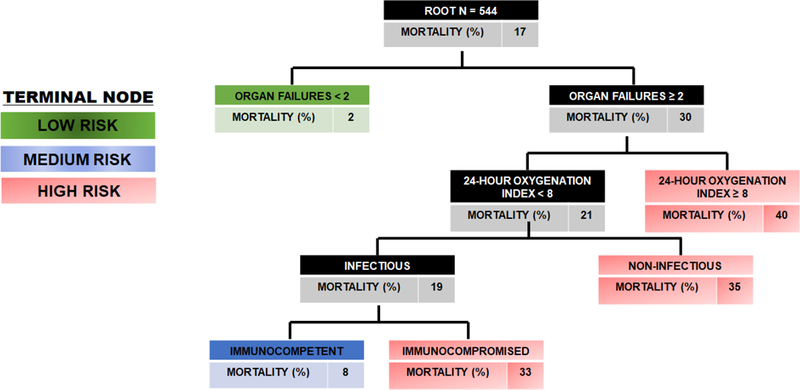
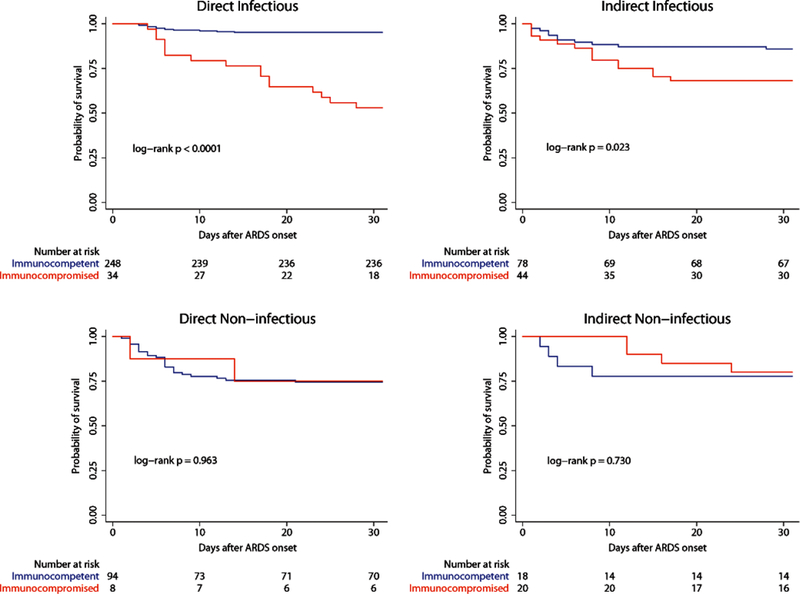
Direct ARDS had lower severity of illness (p < 0.001) but worse oxygenation (p < 0.001), relative to indirect. Predictors of mortality were similar for direct and indirect ARDS. When comparing infectious and non-infectious ARDS, infectious ARDS had lower severity of illness (p < 0.001), worse oxygenation (p = 0.014), and lower mortality (p = 0.013). In multivariable analysis, immunocompromised status demonstrated effect modification between infectious and non-infectious ARDS (p = 0.005 for interaction), with no association with mortality in non-infectious ARDS.
In children, direct and indirect ARDS have distinct clinical characteristics, but similar outcomes and similar predictors of mortality. In contrast, infectious and non-infectious ARDS demonstrate heterogeneity of clinical characteristics, mortality, and predictors of mortality, with traditional predictors of ARDS mortality only applicable to infectious ARDS.
急性呼吸窘迫综合征(ARDS)在病因学上具有异质性,这可能会影响结局。将其分为生物学定义的亚型可能会降低异质性。但是,尚不清楚儿科 ARDS 是否存在具有临床意义的亚型。我们旨在确定直接性和间接性 ARDS 之间以及感染性和非感染性 ARDS 之间的临床特征和死亡率预测因素是否存在差异。
这是一项针对 2011 年 7 月至 2017 年 6 月期间在柏林患有 ARDS 的 544 名儿童的单中心前瞻性队列研究,将其分为直接性 ARDS 与间接性 ARDS,以及感染性 ARDS 与非感染性 ARDS。使用多变量逻辑回归测试整个队列以及亚组内死亡率的预测因素。使用交互检验评估亚组之间的效应修饰。
直接性 ARDS 的疾病严重程度较低(p<0.001),但氧合情况更差(p<0.001),而间接性 ARDS 则相反。直接性 ARDS 和间接性 ARDS 的死亡率预测因素相似。当比较感染性和非感染性 ARDS 时,感染性 ARDS 的疾病严重程度较低(p<0.001),氧合情况更差(p=0.014),死亡率较低(p=0.013)。在多变量分析中,免疫功能低下状态在感染性和非感染性 ARDS 之间显示出效应修饰(p=0.005),与非感染性 ARDS 中的死亡率无关。
在儿童中,直接性和间接性 ARDS 具有不同的临床特征,但结局和死亡率预测因素相似。相反,感染性和非感染性 ARDS 显示出临床特征、死亡率和死亡率预测因素的异质性,ARDS 死亡率的传统预测因素仅适用于感染性 ARDS。