Nora Eccles Harrison Cardiovascular Research and Training Institute, University of Utah, Salt Lake City, Utah, United States of America.
Department of Bioengineering, University of Utah, Salt Lake City, Utah, United States of America.
PLoS One. 2018 Jul 5;13(7):e0200301. doi: 10.1371/journal.pone.0200301. eCollection 2018.
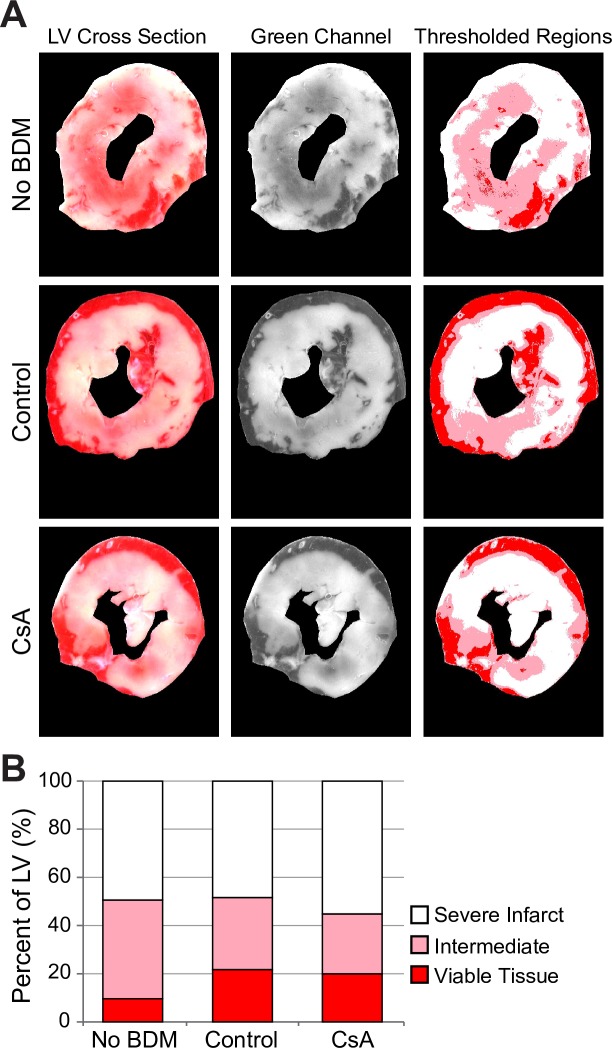
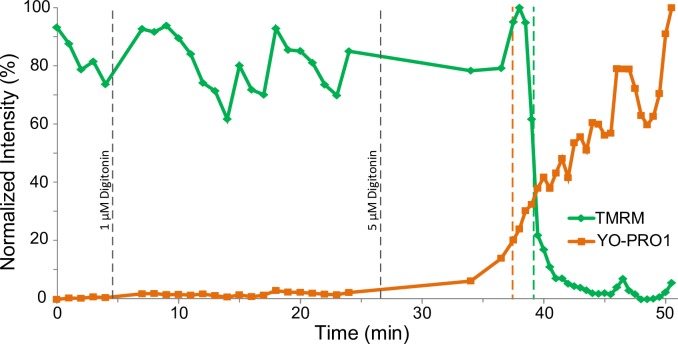
A prominent theory of cell death in myocardial ischemia/reperfusion (I/R) posits that the primary and pivotal step of irreversible cell injury is the opening of the mitochondrial permeability transition (MPT) pore. However, the predominantly positive evidence of protection against infarct afforded by the MPT inhibitor, Cyclosporine A (CsA), in experimental studies is in stark contrast with the overall lack of benefit found in clinical trials of CsA. One reason for the discrepancy might be the fact that relatively short experimental ischemic episodes (<1 hour) do not represent clinically-realistic durations, usually exceeding one hour. Here we tested the hypothesis that MPT is not the primary event of cell death after prolonged (60-80 min) episodes of global ischemia. We used confocal microcopy in Langendorff-perfused rabbit hearts treated with the electromechanical uncoupler, 2,3-Butanedione monoxime (BDM, 20 mM) to allow tracking of MPT and sarcolemmal permeabilization (SP) in individual ventricular myocytes. The time of the steepest drop in fluorescence of mitochondrial membrane potential (ΔΨm)-sensitive dye, TMRM, was used as the time of MPT (TMPT). The time of 20% uptake of the normally cell-impermeable dye, YO-PRO1, was used as the time of SP (TSP). We found that during reperfusion MPT and SP were tightly coupled, with MPT trending slightly ahead of SP (TSP-TMPT = 0.76±1.31 min; p = 0.07). These coupled MPT/SP events occurred in discrete myocytes without crossing cell boundaries. CsA (0.2 μM) did not reduce the infarct size, but separated SP and MPT events, such that detectable SP was significantly ahead of MPT (TSP -TMPT = -1.75±1.28 min, p = 0.006). Mild permeabilization of cells with digitonin (2.5-20 μM) caused coupled MPT/SP events which occurred in discrete myocytes similar to those observed in Control and CsA groups. In contrast, deliberate induction of MPT by titration with H2O2 (200-800 μM), caused propagating waves of MPT which crossed cell boundaries and were uncoupled from SP. Taken together, these findings suggest that after prolonged episodes of ischemia, SP is the primary step in myocyte death, of which MPT is an immediate and unavoidable consequence.
一种关于心肌缺血/再灌注(I/R)中细胞死亡的突出理论认为,线粒体通透性转换(MPT)孔的开放是不可逆细胞损伤的主要和关键步骤。然而,在实验研究中,MPT 抑制剂环孢菌素 A(CsA)提供的对梗塞的保护主要是阳性证据,与 CsA 的临床试验中总体缺乏益处形成鲜明对比。造成这种差异的一个原因可能是相对较短的实验性缺血发作(<1 小时)不能代表临床上现实的持续时间,通常超过 1 小时。在这里,我们测试了以下假设:在长时间(60-80 分钟)的全缺血发作后,MPT 不是细胞死亡的主要事件。我们使用 Langendorff 灌注兔心脏中的共聚焦显微镜,用电子机械解偶联剂 2,3-丁二酮单肟(BDM,20 mM)处理,以跟踪单个心室肌细胞中的 MPT 和肌浆膜通透性(SP)。线粒体膜电位(ΔΨm)敏感染料 TMRM 荧光急剧下降的时间用作 MPT(TMPT)的时间。正常情况下细胞不可渗透的染料 YO-PRO1 摄取 20%的时间用作 SP(TSP)的时间。我们发现,在再灌注期间,MPT 和 SP 紧密偶联,MPT 略微领先于 SP(TSP-TMPT = 0.76±1.31 分钟;p = 0.07)。这些偶联的 MPT/SP 事件发生在没有穿过细胞边界的离散肌细胞中。CsA(0.2 μM)并未减少梗塞面积,但将 SP 和 MPT 事件分开,使得可检测到的 SP 明显早于 MPT(TSP-TMPT = -1.75±1.28 分钟,p = 0.006)。用二氢月桂基硫酸钠(2.5-20 μM)轻度透化细胞会导致偶联的 MPT/SP 事件,这些事件发生在与对照和 CsA 组中观察到的离散肌细胞中类似的离散肌细胞中。相比之下,通过用 H2O2(200-800 μM)滴定诱导 MPT,会导致 MPT 的传播波穿过细胞边界,与 SP 解偶联。总之,这些发现表明,在长时间的缺血发作后,SP 是肌细胞死亡的主要步骤,而 MPT 是其立即且不可避免的后果。