Barnes Thomas R E, Leeson Verity, Paton Carol, Marston Louise, Osborn David P, Kumar Raj, Keown Patrick, Zafar Rameez, Iqbal Khalid, Singh Vineet, Fridrich Pavel, Fitzgerald Zachary, Bagalkote Hemant, Haddad Peter M, Husni Mariwan, Amos Tim
Centre for Psychiatry, Hammersmith Hospital Campus, Imperial College London, 7th Floor Commonwealth Building, Du Cane Road, London W12 0NN, UK.
Centre for Psychiatry, Imperial College London, UK.
Ther Adv Psychopharmacol. 2018 Jul;8(7):185-197. doi: 10.1177/2045125318762365. Epub 2018 Mar 8.
A second antipsychotic is commonly added to clozapine to treat refractory schizophrenia, notwithstanding the limited evidence to support such practice.
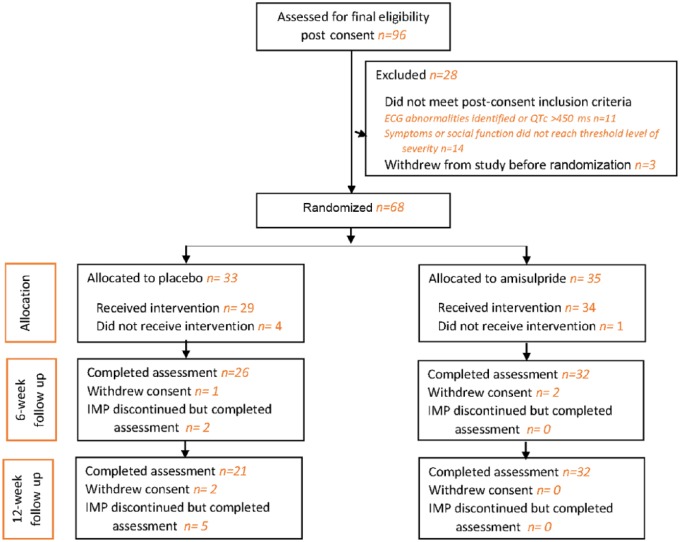
The efficacy and adverse effects of this pharmacological strategy were examined in a double-blind, placebo-controlled, 12-week randomized trial of clozapine augmentation with amisulpride, involving 68 adults with treatment-resistant schizophrenia and persistent symptoms despite a predefined trial of clozapine.
There were no statistically significant differences between the amisulpride and placebo groups on the primary outcome measure (clinical response defined as a 20% reduction in total Positive and Negative Syndrome Scale score) or other mental state measures. However, the trial under recruited and was therefore underpowered to detect differences in the primary outcome, meaning that acceptance of the null hypothesis carries an increased risk of type II error. The findings suggested that amisulpride-treated participants were more likely to fulfil the clinical response criterion, odds ratio 1.17 (95% confidence interval 0.40-3.42) and have a greater reduction in negative symptoms, but these numerical differences were not statistically significant and only evident at 12 weeks. A significantly higher proportion of participants in the amisulpride group had at least one adverse event compared with the control group ( = 0.014), and these were more likely to be cardiac symptoms.
Treatment for more than 6 weeks may be required for an adequate trial of clozapine augmentation with amisulpride. The greater side-effect burden associated with this treatment strategy highlights the need for safety and tolerability monitoring, including vigilance for indicators of cardiac abnormalities, when it is used in either a clinical or research setting.
尽管支持这种做法的证据有限,但通常会在氯氮平基础上加用第二种抗精神病药物来治疗难治性精神分裂症。
在一项双盲、安慰剂对照、为期12周的随机试验中,研究了这种药物治疗策略的疗效和不良反应,该试验为氯氮平联合氨磺必利增效治疗,纳入68例对治疗有抵抗且在经过预定义的氯氮平试验后仍有持续症状的成年精神分裂症患者。
在主要结局指标(临床反应定义为阳性和阴性症状量表总分降低20%)或其他精神状态指标方面,氨磺必利组和安慰剂组之间无统计学显著差异。然而,该试验招募不足,因此检测主要结局差异的效能不足,这意味着接受零假设会增加II型错误的风险。研究结果表明,接受氨磺必利治疗的参与者更有可能达到临床反应标准,比值比为1.17(95%置信区间0.40 - 3.42),且阴性症状有更大程度的减轻,但这些数值差异无统计学显著性,且仅在12周时明显。与对照组相比,氨磺必利组中至少发生一次不良事件的参与者比例显著更高(P = 0.014),且这些不良事件更可能是心脏症状。
氯氮平联合氨磺必利增效治疗可能需要超过6周的时间进行充分试验。这种治疗策略带来的更大副作用负担凸显了在临床或研究环境中使用时进行安全性和耐受性监测的必要性,包括警惕心脏异常指标。