Erin Trish (
Jianhui Xu is a doctoral student at the Price School of Public Policy and the Leonard D. Schaeffer Center for Health Policy and Economics, University of Southern California.
Health Aff (Millwood). 2018 Jul;37(7):1048-1056. doi: 10.1377/hlthaff.2018.0006.
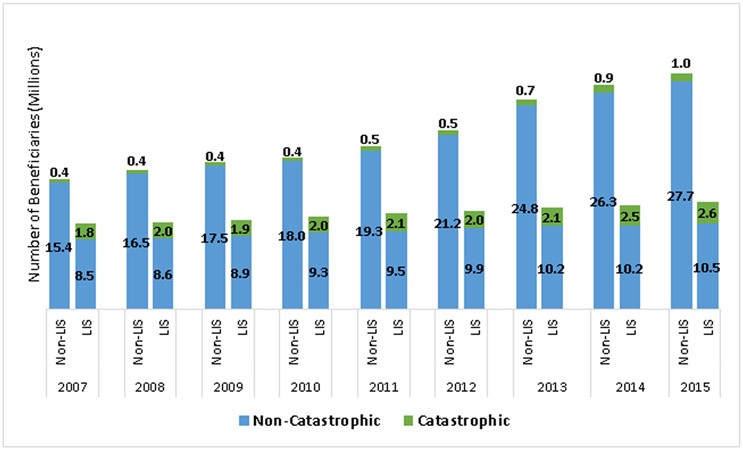
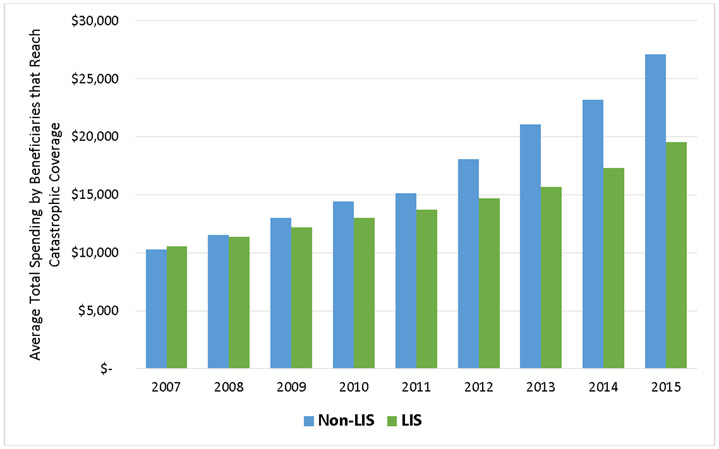
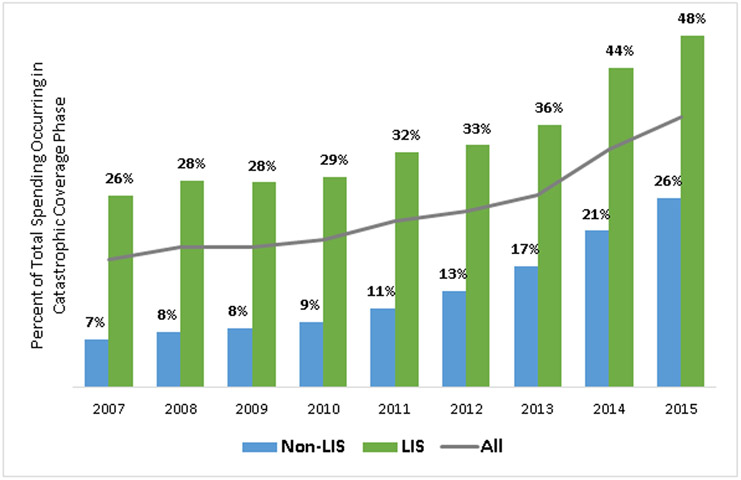
Medicare Part D has no cap on beneficiaries' out-of-pocket spending for outpatient prescription drugs, and, unlike Medicare Parts A and B, beneficiaries are prohibited from purchasing supplemental insurance that could provide such a cap. Historically, most beneficiaries whose annual Part D spending reached the catastrophic level were protected from unlimited personal liability by the Low-Income Subsidy (LIS). However, we found that the proportion of beneficiaries whose spending reached that level but did not qualify for the subsidy-and therefore remained liable for coinsurance-increased rapidly, from 18 percent in 2007 to 28 percent in 2015. Moreover, average total per person per year spending grew much more rapidly for those who did not qualify for the LIS than for those who did, primarily because of differences in price and utilization trends for the drugs that represented disproportionately large shares of their spending. We estimated that a cap for all Part D enrollees in 2015 would have raised monthly premiums by only $0.40-$1.31 per member.
医疗保险 Part D 对门诊处方药的自付费用没有上限,与医疗保险 A 部分和 B 部分不同,受益人不得购买可以提供此类上限的补充保险。从历史上看,大多数年度 Part D 支出达到灾难性水平的受益人通过低收入补贴 (LIS) 免受无限个人责任的保护。然而,我们发现,支出达到这一水平但不符合补贴条件的受益人的比例(因此仍需承担共付额)迅速增加,从 2007 年的 18%增加到 2015 年的 28%。此外,对于那些不符合 LIS 条件的人来说,人均年总支出的增长速度远远快于那些符合条件的人,这主要是由于代表其支出不成比例的大部分药物的价格和使用趋势存在差异。我们估计,2015 年对所有 Part D 参保人设定上限,每个参保人每月只需增加 0.40 美元至 1.31 美元的保费。