Department of Haematology-Oncology, National University Cancer Institute, Singapore, Singapore.
Cancer Science Institute of Singapore, National University of Singapore, Singapore, Singapore.
BMC Med. 2018 Jul 10;16(1):104. doi: 10.1186/s12916-018-1093-8.
Genotype-guided warfarin dosing has been shown in some randomized trials to improve anticoagulation outcomes in individuals of European ancestry, yet its utility in Asian patients remains unresolved.
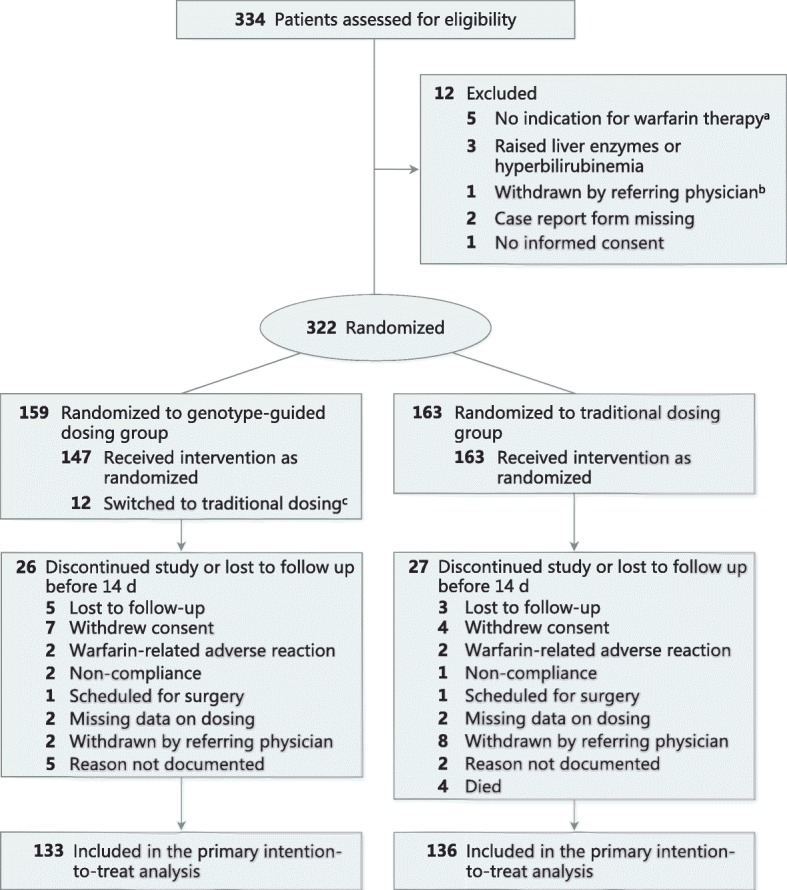
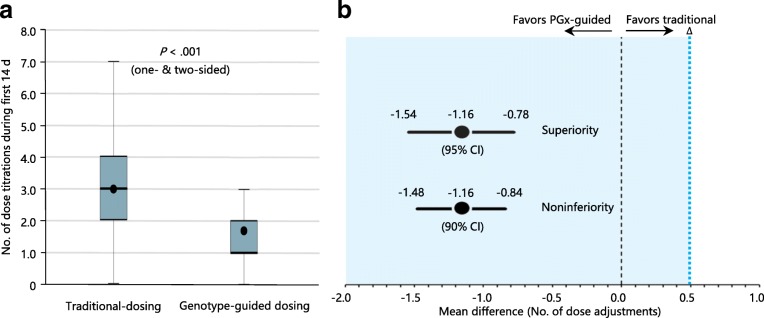
An open-label, non-inferiority, 1:1 randomized trial was conducted at three academic hospitals in South East Asia, involving 322 ethnically diverse patients newly indicated for warfarin (NCT00700895). Clinical follow-up was 90 days. The primary efficacy measure was the number of dose titrations within the first 2 weeks of therapy, with a mean non-inferiority margin of 0.5 over the first 14 days of therapy.
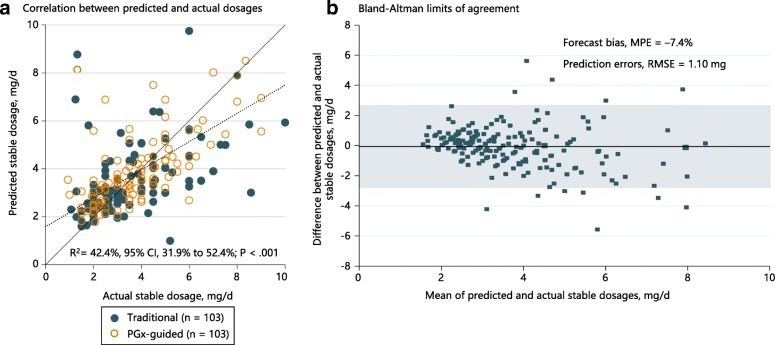
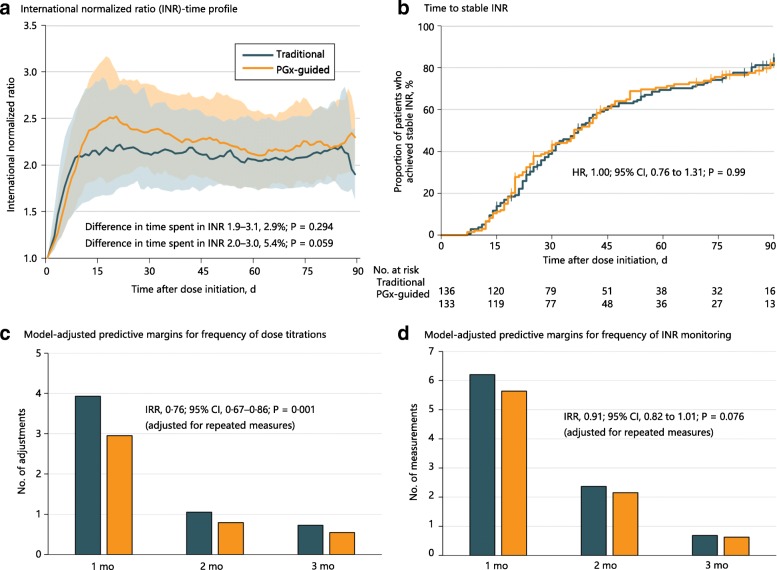
Among 322 randomized patients, 269 were evaluable for the primary endpoint. Compared with traditional dosing, the genotype-guided group required fewer dose titrations during the first 2 weeks (1.77 vs. 2.93, difference -1.16, 90% CI -1.48 to -0.84, P < 0.001 for both non-inferiority and superiority). The percentage of time within the therapeutic range over 3 months and median time to stable international normalized ratio (INR) did not differ between the genotype-guided and traditional dosing groups. The frequency of dose titrations (incidence rate ratio 0.76, 95% CI 0.67 to 0.86, P = 0.001), but not frequency of INR measurements, was lower at 1, 2, and 3 months in the genotype-guided group. The proportions of patients who experienced minor or major bleeding, recurrent venous thromboembolism, or out-of-range INR did not differ between both arms. For predicting maintenance doses, the pharmacogenetic algorithm achieved an R = 42.4% (P < 0.001) and mean percentage error of -7.4%.
Among Asian adults commencing warfarin therapy, a pharmacogenetic algorithm meets criteria for both non-inferiority and superiority in reducing dose titrations compared with a traditional dosing approach, and performs well in prediction of actual maintenance doses. These findings imply that clinicians may consider applying a pharmacogenetic algorithm to personalize initial warfarin dosages in Asian patients.
ClinicalTrials.gov NCT00700895 . Registered on June 19, 2008.
在一些随机试验中,基因型指导的华法林剂量调整已被证明可改善欧洲血统个体的抗凝治疗结果,但在亚洲患者中的应用仍未得到解决。
在东南亚的三家学术医院进行了一项开放标签、非劣效性、1:1 随机试验,共纳入 322 名新接受华法林治疗的种族多样化患者(NCT00700895)。临床随访 90 天。主要疗效指标是治疗前 2 周内的剂量调整次数,治疗前 14 天的平均非劣效性边界为 0.5。
在 322 名随机患者中,269 名患者可评估主要终点。与传统剂量相比,基因型指导组在前 2 周内需要更少的剂量调整(1.77 与 2.93,差值 -1.16,90%CI-1.48 至-0.84,P<0.001 均为非劣效性和优效性)。3 个月内治疗范围内的时间百分比和稳定国际标准化比值(INR)中位数时间在基因型指导组和传统剂量组之间无差异。在基因型指导组中,1、2 和 3 个月时剂量调整的频率(发生率比 0.76,95%CI0.67 至 0.86,P=0.001)而不是 INR 测量的频率较低。两组患者的轻微或大出血、复发性静脉血栓栓塞或 INR 范围外的比例无差异。对于预测维持剂量,药物遗传学算法的 R=42.4%(P<0.001)和平均百分比误差为-7.4%。
在开始华法林治疗的亚洲成年人中,与传统剂量相比,药物遗传学算法在减少剂量调整方面既具有非劣效性又具有优效性,并且在预测实际维持剂量方面表现良好。这些发现表明,临床医生可以考虑在亚洲患者中应用药物遗传学算法来个性化初始华法林剂量。
ClinicalTrials.gov NCT00700895。注册于 2008 年 6 月 19 日。