Hematology/Oncology.
Helen Diller Family Comprehensive Cancer Center.
Blood Adv. 2018 Jul 10;2(13):1595-1607. doi: 10.1182/bloodadvances.2017014845.
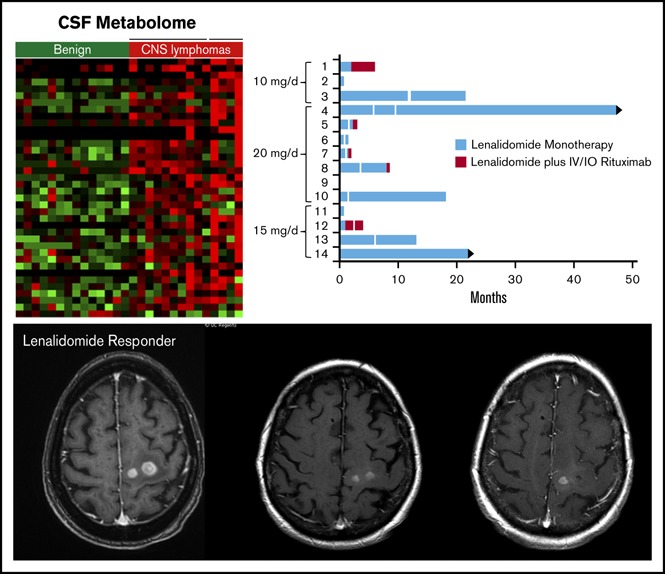
There is an unmet need for effective biological therapies for relapsed central nervous system (CNS) lymphoma. Lenalidomide is active in activated B-cell type diffuse large B-cell lymphoma and rituximab is effective in CNS lymphoma. These observations are the basis for this first trial of an immunomodulatory drug as monotherapy in CNS lymphoma, and, in patients with inadequate responses to lenalidomide, with rituximab. In an independent cohort, we evaluated lenalidomide maintenance after salvage with high-dose methotrexate or focal irradiation in relapsed primary CNS lymphoma (PCNSL). We determined safety, efficacy, and cerebrospinal fluid (CSF) penetration of lenalidomide at 10-, 15-, and 20-mg dose levels in 14 patients with refractory CD20 CNS lymphoma. Nine subjects with relapsed, refractory CNS lymphoma achieved better than partial response with lenalidomide monotherapy, 6 maintained response ≥9 months, and 4 maintained response ≥18 months. Median progression-free survival for lenalidomide/rituximab was 6 months. In the independent cohort, response duration with lenalidomide maintenance after complete responses 2 through 5 were significantly longer than response durations after standard therapy. The CSF/plasma partition coefficient of lenalidomide was ≥20% at 15- and 20-mg dose levels. Change in CSF interleukin-10 at 1 month correlated with clinical response and response duration to lenalidomide. Metabolomic profiling of CSF identified novel biomarkers, including lactate, and implicated indoleamine-2,3 dioxygenase activity with CNS lymphoma progression on lenalidomide. We conclude that lenalidomide penetrates ventricular CSF and is active as monotherapy in relapsed CNS lymphomas. We provide evidence that maintenance lenalidomide potentiates response duration after salvage in relapsed PCNSL and delays whole brain radiotherapy (WBRT). This trial was registered at www.clinicaltrials.gov as #NCT01542918.
中枢神经系统(CNS)淋巴瘤复发患者仍存在未满足的有效生物治疗需求。来那度胺对激活 B 细胞型弥漫大 B 细胞淋巴瘤有效,利妥昔单抗对 CNS 淋巴瘤有效。这些观察结果为这项 CNS 淋巴瘤中免疫调节剂单药治疗的首次试验以及在来那度胺应答不足的患者中联合利妥昔单抗治疗提供了依据。在一个独立队列中,我们评估了在复发原发性 CNS 淋巴瘤(PCNSL)患者中挽救治疗后接受高剂量甲氨蝶呤或局部放疗后使用来那度胺维持治疗的情况。我们在 14 例难治性 CD20 CNS 淋巴瘤患者中评估了来那度胺在 10、15 和 20mg 剂量水平的安全性、疗效和脑脊液(CSF)穿透性。9 例复发、难治性 CNS 淋巴瘤患者接受来那度胺单药治疗后获得优于部分缓解的疗效,6 例维持缓解≥9 个月,4 例维持缓解≥18 个月。来那度胺/利妥昔单抗的中位无进展生存期为 6 个月。在独立队列中,完全缓解 2 至 5 后接受来那度胺维持治疗的缓解持续时间明显长于标准治疗后的缓解持续时间。来那度胺的 CSF/血浆分配系数在 15 和 20mg 剂量水平时≥20%。1 个月时 CSF 白细胞介素-10 的变化与来那度胺的临床反应和缓解持续时间相关。CSF 代谢组学分析确定了新的生物标志物,包括乳酸,并提示吲哚胺 2,3 双加氧酶活性与来那度胺治疗期间 CNS 淋巴瘤进展相关。我们得出结论,来那度胺可穿透脑室 CSF,并作为复发性 CNS 淋巴瘤的单药治疗有效。我们提供的证据表明,在复发 PCNSL 中,维持来那度胺可增强挽救治疗后的缓解持续时间,并延迟全脑放疗(WBRT)。该试验在 www.clinicaltrials.gov 上注册,编号为 NCT01542918。