Tanase Yasuhito, Takahama Junko, Kawaguchi Ryuji, Kobayashi Hiroshi
Department of Obstetrics and Gynecology, Nara Medical University, Kashihara, Nara, Japan.
Department of Radiology, Nara Medical University, Kashihara, Nara, Japan.
World J Oncol. 2018 Jun;9(3):74-79. doi: 10.14740/wjon1106w. Epub 2018 Jun 26.
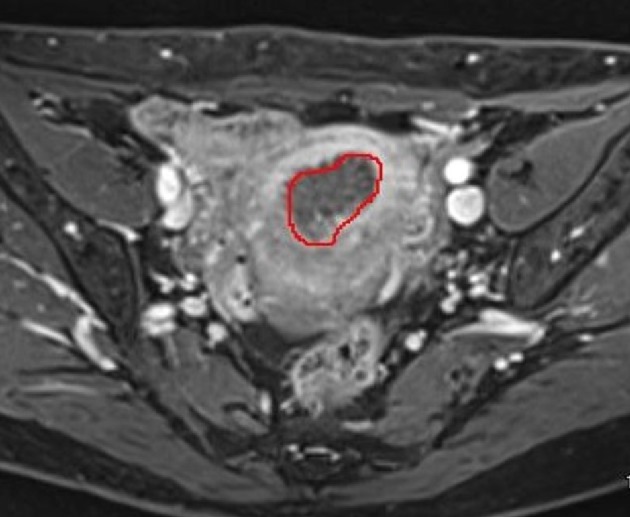
The aim of our study was to evaluate the utility of three-dimensional magnetic resonance imaging (3D-MRI) in gynecologic fields. We examined the relation between tumor volume measured with 3D-MRI and lymph node metastasis in patients with endometrial carcinoma.
A retrospective analysis of 84 patients with endometrial carcinoma who underwent hysterectomy, bilateral salpingo-oophorectomy with pelvic/para-aortic lymphadenectomy at our institute was performed. Of these, the tumor volume of 59 patients could be calculated using 3D-MRI. Age, serum CA125 level, histologic type and grade, volume of tumors were examined in relation to pelvic/para-aortic lymph node metastasis as preoperative risk factors. Tumor volume measurements were calculated using 3D-MRI with AqariusNET Server 4G software. Univariate and multivariate associations between the preoperative risk factors and pelvic/para-aortic lymph node metastasis were analyzed. Receiver operating characteristic (ROC) curves were used to determine the best cut-off points for CA125 levels and tumor volume to predict lymph metastasis.
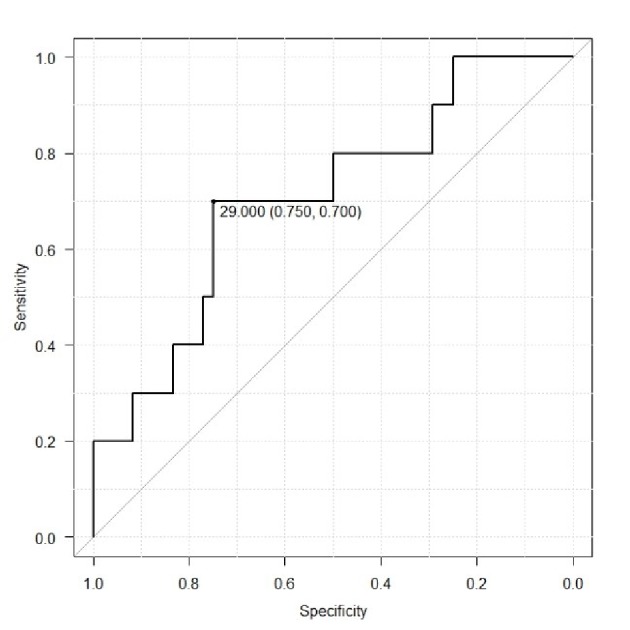
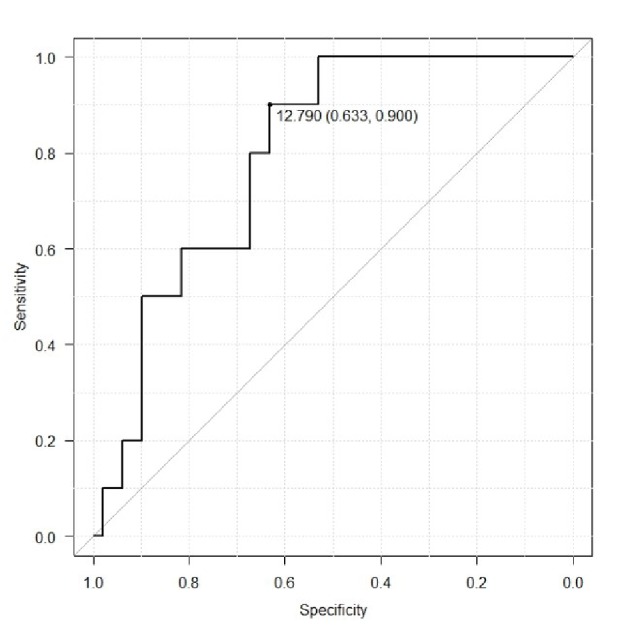
The mean age, CA125 value and tumor volume were 61.6 years, 51.6 (IU/L) and 11.6 (cm), respectively. Lymphatic metastasis occurred in 16.0% (10 of 59) patients. Univariate analysis indicated that a high CA125 level and a tumor volume were risk factors (P = 0.0111, 0.0123 respectively). Multivariate analysis revealed that tumor volume was an independent risk factor for lymphatic metastasis (hazard ratio (HR) 12.7, 95% CI 1.06 - 154). The potential cut-off values of CA-125 level and tumor volume were 29 IU/L (sensitivity: 0.744; specificity: 0.821) and 12.79 cm (sensitivity: 0.821; specificity: 0.744), respectively.
Our results suggest that tumor volume calculated with 3D-MRI correlates with lymph node metastasis in endometrial carcinoma.
我们研究的目的是评估三维磁共振成像(3D-MRI)在妇科领域的应用价值。我们研究了子宫内膜癌患者中通过3D-MRI测量的肿瘤体积与淋巴结转移之间的关系。
对我院84例行子宫切除术、双侧输卵管卵巢切除术及盆腔/腹主动脉旁淋巴结清扫术的子宫内膜癌患者进行回顾性分析。其中,59例患者的肿瘤体积可通过3D-MRI计算得出。对年龄、血清CA125水平、组织学类型和分级、肿瘤体积等作为术前危险因素与盆腔/腹主动脉旁淋巴结转移的关系进行了研究。使用AqariusNET Server 4G软件通过3D-MRI计算肿瘤体积测量值。分析术前危险因素与盆腔/腹主动脉旁淋巴结转移之间的单因素和多因素关联。采用受试者操作特征(ROC)曲线确定CA125水平和肿瘤体积预测淋巴结转移的最佳截断点。
平均年龄、CA125值和肿瘤体积分别为61.6岁、51.6(IU/L)和11.6(cm)。16.0%(59例中的10例)患者发生淋巴结转移。单因素分析表明,CA125水平高和肿瘤体积是危险因素(P分别为0.0111、0.0123)。多因素分析显示,肿瘤体积是淋巴结转移的独立危险因素(风险比(HR)12.7,95%CI 1.06 - 154)。CA-125水平和肿瘤体积的潜在截断值分别为29 IU/L(敏感性:0.744;特异性:0.821)和12.79 cm(敏感性:0.821;特异性:0.744)。
我们的结果表明,通过3D-MRI计算的肿瘤体积与子宫内膜癌的淋巴结转移相关。