Lan Peng, Wang Shuo-Jia, Shi Qiu-Cheng, Fu Ying, Xu Qing-Ye, Chen Tao, Yu Yun-Xian, Pan Kong-Han, Lin Ling, Zhou Jian-Cang, Yu Yun-Song
Department of Critical Care Medicine, Sir Run Run Shaw Hospital Department of Epidemiology and Health Statistics, School of Public Health Department of Infectious Disease Department of Clinical Laboratory, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, China.
Medicine (Baltimore). 2018 Jul;97(28):e11421. doi: 10.1097/MD.0000000000011421.
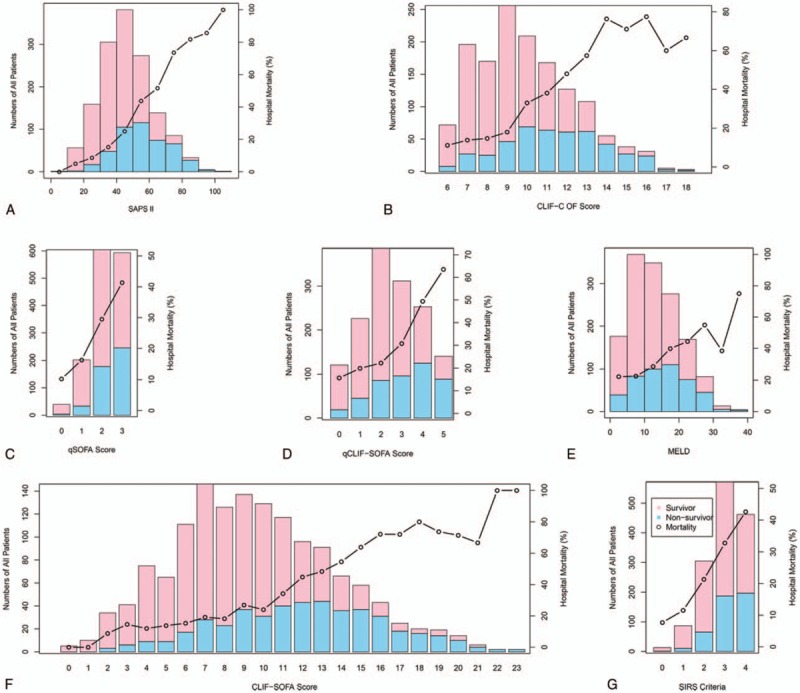
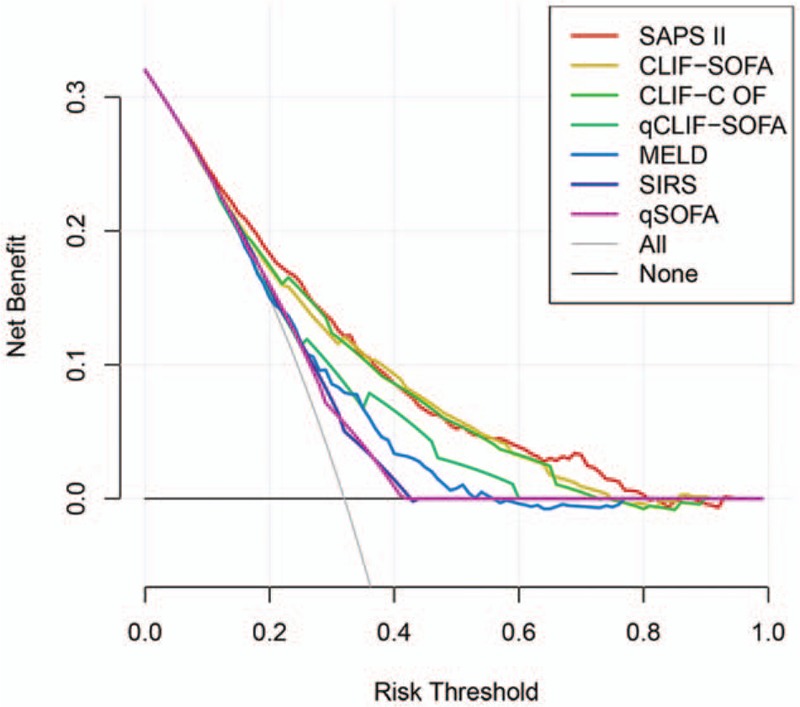
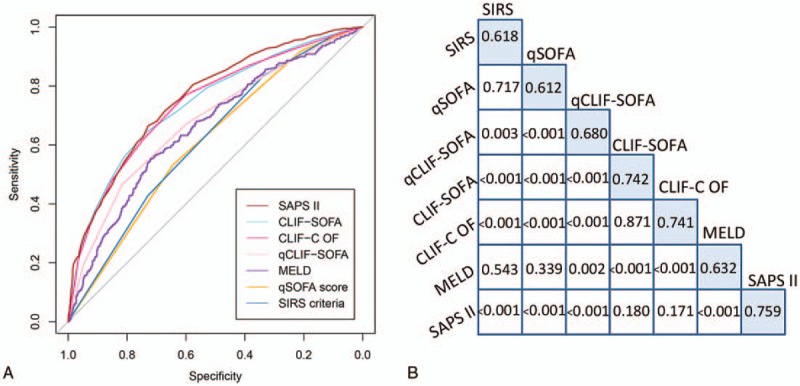
Cirrhotic patients with infection are prone to develop sepsis or even septic shock rendering poorer prognosis. However, few methods are available to predict the prognosis of cirrhotic patients with infection although there are some scoring systems can be used to predict general patients with cirrhosis. Therefore, we aimed to explore the predictive value of scoring systems in determining the outcome of critically ill cirrhotic patients with suspected infection.This was a retrospective cohort study based on a single-center database. The prognostic accuracy of the systemic inflammatory response syndrome (SIRS) criteria, quick Sequential Organ Failure Assessment (qSOFA), chronic liver failure (CLIF)-SOFA, quick CLIF-SOFA (qCLIF-SOFA), CLIF-consortium organ failure (CLIF-C OF), Model for End-Stage Liver Disease (MELD), and Simplified Acute Physiology Score (SAPS) II were compared by using area under the receiver operating characteristic (AUROC) curve and net benefit with decision curve analysis. The primary endpoint was in-hospital mortality while the secondary endpoints were duration of hospital and intensive care unit (ICU) stay and ICU mortality.A total of 1438 cirrhotic patients with suspected infection were included in the study. Nearly half the patients (50.2%) were admitted to the ICU due to hepatic encephalopathy and the overall in-hospital mortality was 32.0%. Hospital and ICU mortality increased as the score of each scoring system increased (P < .05 for all trends). The AUROC of CLIF-SOFA (AUROC, 0.742; 95% confidence interval, CI, 0.714-0.770), CLIF-C OF (AUROC, 0.741; 95% CI, 0.713-0.769), and SAPS II (AUROC, 0.759; 95% CI, 0.733-0.786) were significantly higher than SIRS criteria (AUROC, 0.618; 95% CI, 0.590-0.647), qSOFA (AUROC, 0.612; 95% CI, 0.584-0.640), MELD (AUROC, 0.632; 95% CI, 0.601-0.662), or qCLIF-SOFA (AUROC, 0.680; 95% CI, 0.650-0.710) (P < .05 for all). In the decision curve analysis, the net benefit of implementing CLIF-SOFA and CLIF-C OF to predict the prognosis of cirrhotic patients with suspected infection were higher compared with SIRS, qSOFA, MELD, or qCLIF-SOFA.CLIF-SOFA and CLIF-C OF scores, as well as SAPS II were better tools than SIRS, qSOFA, MELD, or qCLIF-SOFA to evaluate the prognosis of critically ill cirrhotic patients with suspected infection.
感染的肝硬化患者容易发生脓毒症甚至感染性休克,预后较差。然而,尽管有一些评分系统可用于预测一般肝硬化患者的情况,但很少有方法可用于预测感染的肝硬化患者的预后。因此,我们旨在探讨评分系统在确定疑似感染的重症肝硬化患者结局方面的预测价值。
这是一项基于单中心数据库的回顾性队列研究。通过使用受试者工作特征曲线下面积(AUROC)和决策曲线分析的净效益,比较了全身炎症反应综合征(SIRS)标准、快速序贯器官衰竭评估(qSOFA)、慢性肝衰竭(CLIF)-SOFA、快速CLIF-SOFA(qCLIF-SOFA)、CLIF联盟器官衰竭(CLIF-C OF)、终末期肝病模型(MELD)和简化急性生理学评分(SAPS)II的预后准确性。主要终点是住院死亡率,次要终点是住院时间和重症监护病房(ICU)住院时间以及ICU死亡率。
该研究共纳入1438例疑似感染的肝硬化患者。近一半患者(50.2%)因肝性脑病入住ICU,总体住院死亡率为32.0%。随着每个评分系统得分的增加,医院和ICU死亡率均升高(所有趋势P<0.05)。CLIF-SOFA(AUROC,0.742;95%置信区间,CI,0.714-0.770)、CLIF-C OF(AUROC,0.741;95%CI,0.713-0.769)和SAPS II(AUROC,0.759;95%CI,0.733-0.786)的AUROC显著高于SIRS标准(AUROC,0.618;95%CI,0.590-0.647)、qSOFA(AUROC,0.612;95%CI)、0.5多,少,0.640)、MELD(AUROC,0.632;95%CI,0.601-0.662)或qCLIF-SOFA(AUROC,0.680;95%CI,0.650-0.710)(所有P<0.05)。在决策曲线分析中,与SIRS、qSOFA、MELD或qCLIF-SOFA相比,实施CLIF-SOFA和CLIF-C OF预测疑似感染的肝硬化患者预后的净效益更高。
CLIF-SOFA和CLIF-C OF评分以及SAPS II是比SIRS、qSOFA、MELD或qCLIF-SOFA更好的工具,可用于评估疑似感染的重症肝硬化患者的预后。