Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, South Africa.
Military HIV Research Program, Bethesda, Maryland, United States of America.
PLoS Med. 2018 Jul 11;15(7):e1002591. doi: 10.1371/journal.pmed.1002591. eCollection 2018 Jul.
An estimated 32,000 children develop multidrug-resistant tuberculosis (MDR-TB; Mycobacterium tuberculosis resistant to isoniazid and rifampin) each year. Little is known about the optimal treatment for these children.
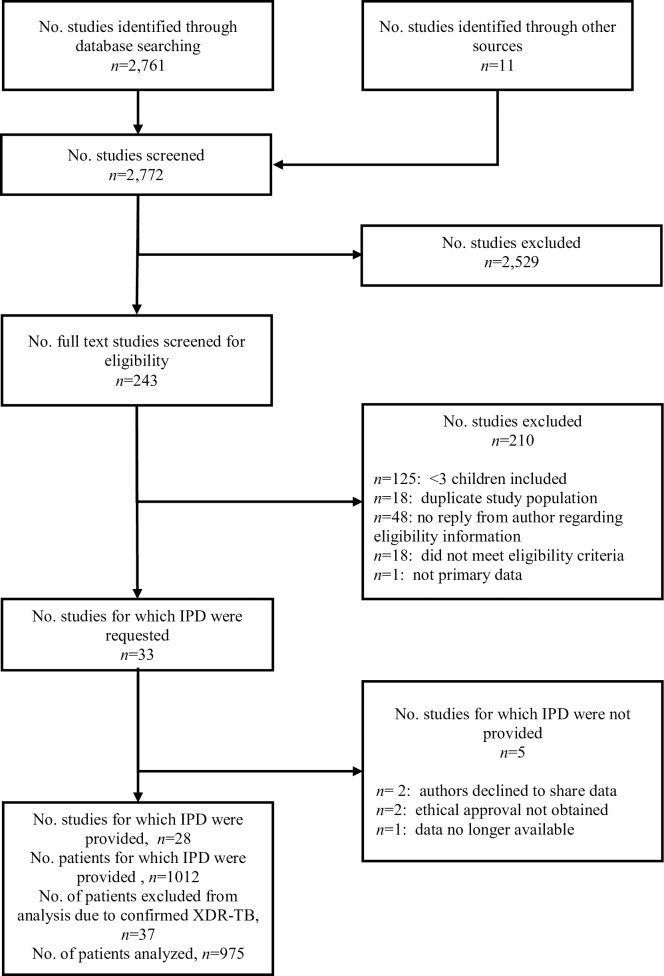
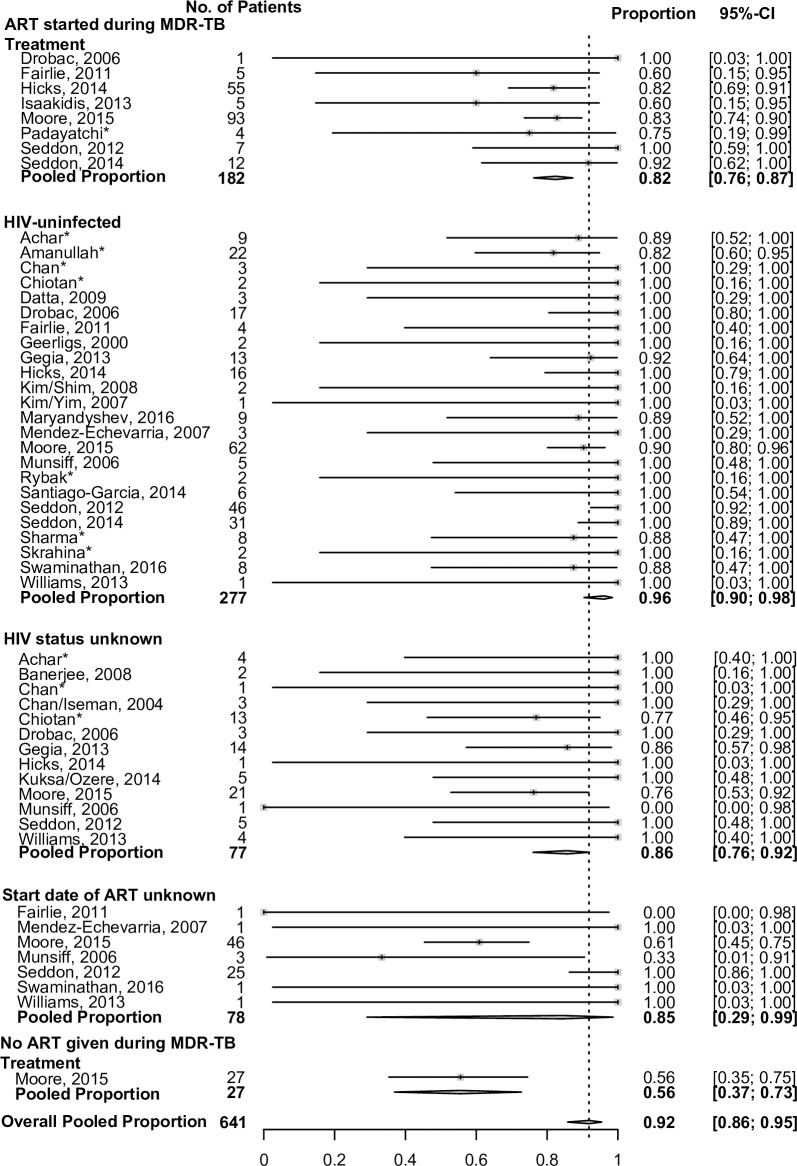
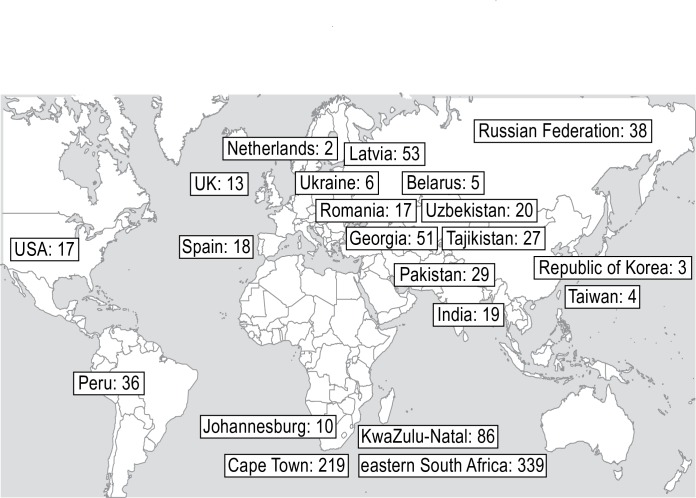
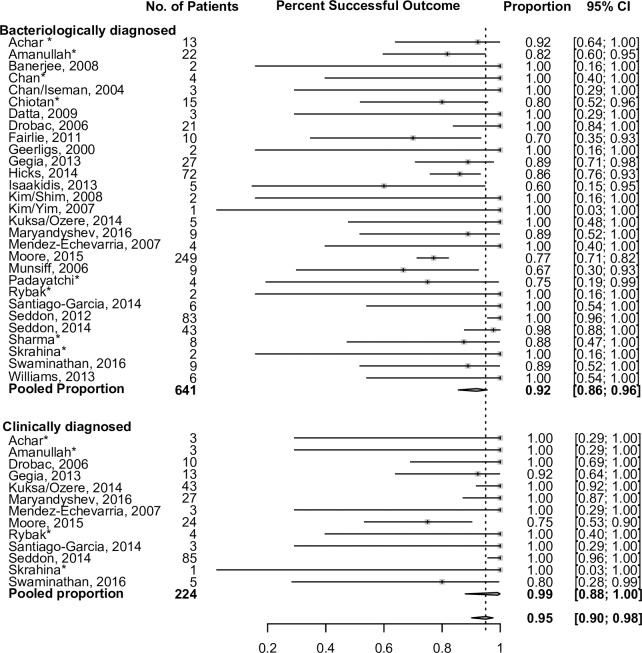
To inform the pediatric aspects of the revised World Health Organization (WHO) MDR-TB treatment guidelines, we performed a systematic review and individual patient data (IPD) meta-analysis, describing treatment outcomes in children treated for MDR-TB. To identify eligible reports we searched PubMed, LILACS, Embase, The Cochrane Library, PsychINFO, and BioMedCentral databases through 1 October 2014. To identify unpublished data, we reviewed conference abstracts, contacted experts in the field, and requested data through other routes, including at national and international conferences and through organizations working in pediatric MDR-TB. A cohort was eligible for inclusion if it included a minimum of three children (aged <15 years) who were treated for bacteriologically confirmed or clinically diagnosed MDR-TB, and if treatment outcomes were reported. The search yielded 2,772 reports; after review, 33 studies were eligible for inclusion, with IPD provided for 28 of these. All data were from published or unpublished observational cohorts. We analyzed demographic, clinical, and treatment factors as predictors of treatment outcome. In order to obtain adjusted estimates, we used a random-effects multivariable logistic regression (random intercept and random slope, unless specified otherwise) adjusted for the following covariates: age, sex, HIV infection, malnutrition, severe extrapulmonary disease, or the presence of severe disease on chest radiograph. We analyzed data from 975 children from 18 countries; 731 (75%) had bacteriologically confirmed and 244 (25%) had clinically diagnosed MDR-TB. The median age was 7.1 years. Of 910 (93%) children with documented HIV status, 359 (39%) were infected with HIV. When compared to clinically diagnosed patients, children with confirmed MDR-TB were more likely to be older, to be infected with HIV, to be malnourished, and to have severe tuberculosis (TB) on chest radiograph (p < 0.001 for all characteristics). Overall, 764 of 975 (78%) had a successful treatment outcome at the conclusion of therapy: 548/731 (75%) of confirmed and 216/244 (89%) of clinically diagnosed children (absolute difference 14%, 95% confidence interval [CI] 8%-19%, p < 0.001). Treatment was successful in only 56% of children with bacteriologically confirmed TB who were infected with HIV who did not receive any antiretroviral treatment (ART) during MDR-TB therapy, compared to 82% in children infected with HIV who received ART during MDR-TB therapy (absolute difference 26%, 95% CI 5%-48%, p = 0.006). In children with confirmed MDR-TB, the use of second-line injectable agents and high-dose isoniazid (15-20 mg/kg/day) were associated with treatment success (adjusted odds ratio [aOR] 2.9, 95% CI 1.0-8.3, p = 0.041 and aOR 5.9, 95% CI 1.7-20.5, p = 0.007, respectively). These findings for high-dose isoniazid may have been affected by site effect, as the majority of patients came from Cape Town. Limitations of this study include the difficulty of estimating the treatment effects of individual drugs within multidrug regimens, only observational cohort studies were available for inclusion, and treatment decisions were based on the clinician's perception of illness, with resulting potential for bias.
This study suggests that children respond favorably to MDR-TB treatment. The low success rate in children infected with HIV who did not receive ART during their MDR-TB treatment highlights the need for ART in these children. Our findings of individual drug effects on treatment outcome should be further evaluated.
每年约有 32000 名儿童罹患耐多药结核病(MDR-TB;对异烟肼和利福平耐药的结核分枝杆菌)。对于这些儿童,最佳的治疗方法尚不清楚。
为了为修订后的世界卫生组织(WHO)耐多药结核病治疗指南提供儿科方面的信息,我们进行了系统评价和个体患者数据(IPD)荟萃分析,描述了接受耐多药结核病治疗的儿童的治疗结果。为了确定符合条件的报告,我们通过 10 月 1 日之前的 PubMed、LILACS、Embase、The Cochrane Library、PsychINFO 和 BioMedCentral 数据库进行了搜索。为了确定未发表的数据,我们查阅了会议摘要,联系了该领域的专家,并通过其他途径请求数据,包括在国家和国际会议上以及在从事儿科耐多药结核病工作的组织中。如果队列至少包括 3 名(年龄<15 岁)经细菌学证实或临床诊断为耐多药结核病的儿童,并且报告了治疗结果,则该队列符合纳入标准。检索结果产生了 2772 份报告;经过审查,有 33 项研究符合纳入标准,其中 28 项提供了 IPD。所有数据均来自已发表或未发表的观察性队列。我们分析了人口统计学、临床和治疗因素作为治疗结果的预测因素。为了获得调整后的估计值,我们使用了随机效应多变量逻辑回归(除非另有说明,否则为随机截距和随机斜率),并调整了以下协变量:年龄、性别、HIV 感染、营养不良、严重肺外疾病或胸部 X 线片上存在严重疾病。我们分析了来自 18 个国家的 975 名儿童的数据;731 名(75%)患儿经细菌学证实,244 名(25%)患儿经临床诊断为耐多药结核病。中位年龄为 7.1 岁。在 910 名(93%)有记录 HIV 状态的儿童中,359 名(39%)感染了 HIV。与临床诊断的患者相比,经细菌学证实的 MDR-TB 患儿更可能年龄较大、感染 HIV、营养不良和胸部 X 线片上有严重结核病(所有特征的 p<0.001)。总体而言,975 名患儿中有 915 名(94%)在治疗结束时取得了成功的治疗结果:731 名(75%)确诊和 244 名(89%)临床诊断患儿(绝对差异为 14%,95%置信区间[CI]为 8%-19%,p<0.001)。在未接受任何抗逆转录病毒治疗(ART)的 HIV 感染患儿中,经细菌学证实的结核病患儿的治疗成功率仅为 56%,而在接受 ART 的 HIV 感染患儿中为 82%(绝对差异为 26%,95%CI 为 5%-48%,p=0.006)。在确诊为 MDR-TB 的患儿中,使用二线注射药物和高剂量异烟肼(15-20mg/kg/天)与治疗成功相关(调整后比值比[aOR]为 2.9,95%CI 为 1.0-8.3,p=0.041;aOR 为 5.9,95%CI 为 1.7-20.5,p=0.007)。高剂量异烟肼的这些发现可能受到了来自开普敦的站点效应的影响,因为大多数患儿都来自那里。本研究的局限性包括在多药方案中估计个别药物治疗效果的困难、仅可获得纳入的观察性队列研究以及治疗决策基于临床医生对疾病的认知,因此可能存在偏倚。
本研究表明,儿童对耐多药结核病治疗反应良好。在未接受 ART 治疗的 HIV 感染患儿中,治疗成功率较低,这突显了这些患儿需要接受 ART。我们对治疗结果中个别药物作用的发现应进一步评估。