Institut Pierre Louis d'épidémiologie et de Santé Publique (IPLESP UMRS 1136), Sorbonne Universités, INSERM, UPMC Univ Paris 06, F75013, Paris, France.
INSERM-TRANSFERT, Paris, France.
BMC Infect Dis. 2018 Jul 11;18(1):326. doi: 10.1186/s12879-018-3231-5.
Etravirine (ETR), a non-nucleoside reverse transcriptase inhibitor (NNRTI) available in France since 2006, is indicated for antiretroviral-experienced HIV-infected adults, in combination with a ritonavir-boosted protease inhibitor (PI). To assess its clinical impact in routine care, we compared hospitalization rates according to ETR + PI prescription or not, among heavily treated HIV-1 infected individuals on failing regimens between 2005 and 2011.
From the French Hospital Database on HIV (ANRS CO4), we selected heavily treated individuals (prior exposure to at least 2 nucleoside reverse transcriptase inhibitor (NRTI), 2PI and 1 NNRTI) with viral load (VL) > 50 copies/mL who started a new antiretroviral (ARV) regimen between 2005 and 2011. Using an intention-to-continue-treatment approach, hospitalization rates were calculated for the individuals who received ETR + PI, during the months after initiating ETR + PI (ETR + PI) or for the individuals who received ETR + PI, in the months before ETR + PI initiation and for the individuals who never received ETR + PI (no ETR + PI). hospitalization from an AIDS-defining cause and hospitalization from a non-AIDS defining cause rates were also calculated. Poisson regression models were used to compare the incidences between the two groups, with adjustment for potential confounders.
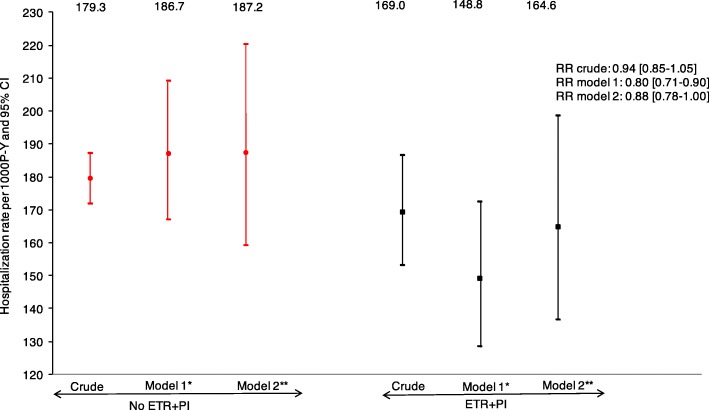
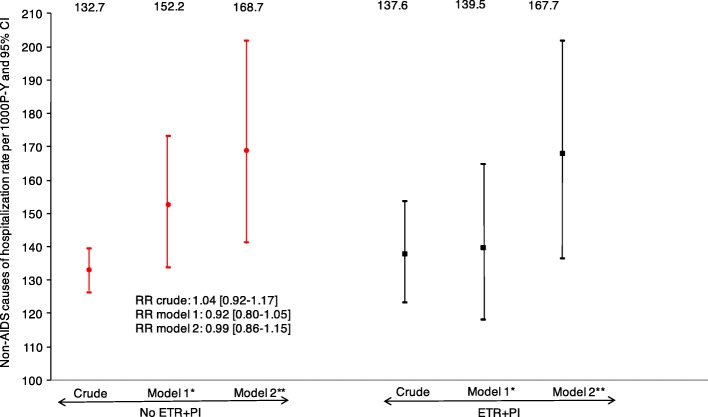
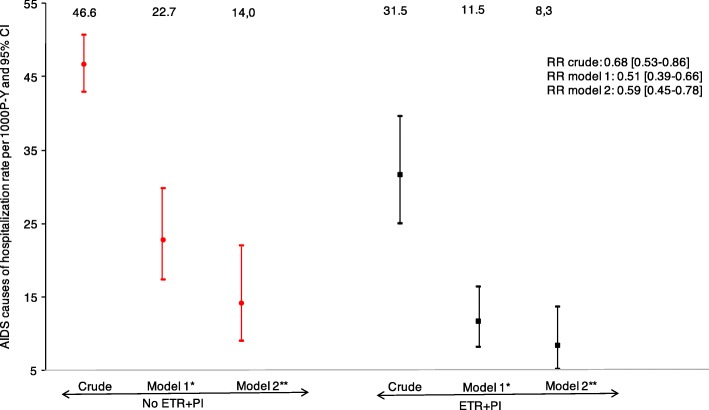
Of 3884 patients who met the inclusion criteria, 838 (21.6%) received ETR + PI. During 13,986 person-years (P-Y) of follow-up, there were 2484 hospitalizations in 956 individuals. The hospitalization rates per 1000 P-Y were 169.0 among individuals exposed to ETR + PI and 179.3 among those not exposed to ETR + PI. After adjustment, the respective hospitalization rates were 148.8 and 186.7 per 1000 P-Y, with an estimated relative risk of 0.80 (95%CI: 0.71-0.90), AIDS hospitalization rates were 11.5 and 22.7 per 1000 P-Y, with an estimated relative risk of 0.51(95%CI: 0.39-0.66) and non-AIDS hospitalization rates were 139.5 and 152.2 per 1000 P-Y, with an estimated relative risk of 0.92 (95%CI: 0.80-1.05).
Between 2005 and 2011, access to ETR + PI was associated with a 20% reduction in the hospitalization rate among heavily treated HIV-1-infected individuals. This reduction was mainly due to a reduction in the AIDS hospitalization rate.
依曲韦林(ETR)是一种自 2006 年起在法国上市的非核苷类逆转录酶抑制剂(NNRTI),适用于有抗逆转录病毒治疗史的 HIV 感染成人,与利托那韦增效蛋白酶抑制剂(PI)联合使用。为了评估其在常规护理中的临床影响,我们比较了 2005 年至 2011 年间治疗方案失败的大量接受治疗的 HIV-1 感染者中,依曲韦林+PI 处方与未处方依曲韦林+PI 的住院率。
我们从法国艾滋病医院数据库(ANRS CO4)中选择了大量接受治疗的个体(至少接受过 2 种核苷逆转录酶抑制剂(NRTI)、2 种 PI 和 1 种 NNRTI 治疗),病毒载量(VL)>50 拷贝/ml,他们在 2005 年至 2011 年期间开始了新的抗逆转录病毒(ARV)治疗方案。采用意向治疗方法,计算了开始使用依曲韦林+PI 后几个月内(ETR+PI 期间)接受依曲韦林+PI 的个体、开始使用依曲韦林+PI 前几个月内接受依曲韦林+PI 的个体和从未接受过依曲韦林+PI 的个体(无 ETR+PI)的住院率。还计算了艾滋病定义性疾病和非艾滋病定义性疾病的住院率。使用泊松回归模型比较了两组的发病率,同时调整了潜在混杂因素。
在符合纳入标准的 3884 名患者中,838 名(21.6%)接受了依曲韦林+PI。在 13986 人年(P-Y)的随访期间,956 名患者中有 2484 人住院。每 1000 P-Y 的住院率分别为接受 ETR+PI 治疗的个体为 169.0 例和未接受 ETR+PI 治疗的个体为 179.3 例。调整后,相应的住院率分别为每 1000 P-Y 148.8 和 186.7,估计相对风险为 0.80(95%CI:0.71-0.90),艾滋病住院率分别为每 1000 P-Y 11.5 和 22.7,估计相对风险为 0.51(95%CI:0.39-0.66),非艾滋病住院率分别为每 1000 P-Y 139.5 和 152.2,估计相对风险为 0.92(95%CI:0.80-1.05)。
2005 年至 2011 年间,获得依曲韦林+PI 治疗与大量接受治疗的 HIV-1 感染者的住院率降低 20%有关。这种降低主要是由于艾滋病住院率的降低。