Institute of Clinical Medicine, National Yang-Ming University, Taipei, Taiwan.
Cardiovascular Research Center, National Yang-Ming University, Taipei, Taiwan.
J Immunother Cancer. 2018 Jul 16;6(1):72. doi: 10.1186/s40425-018-0388-9.
Use of anti-programmed cell death-1 (anti-PD-1) has been successful in treating many types of cancers. Despite its promising efficacy, immune-related adverse events are still a major concern. Immune-related cardiotoxicity, which is rare but fatal, has recently become a focus of attention. Cardiotoxicities including myocarditis, cardiomyopathy, cardiac fibrosis, heart block and cardiac arrest have been reported. Of these toxicities, myocarditis is often accompanied by dysrhythmia. The presentation of sick sinus syndrome as an immune-related adverse event has not yet been reported. Here, we reported the first case of sick sinus syndrome, a rare toxicity induced by anti-PD-1.
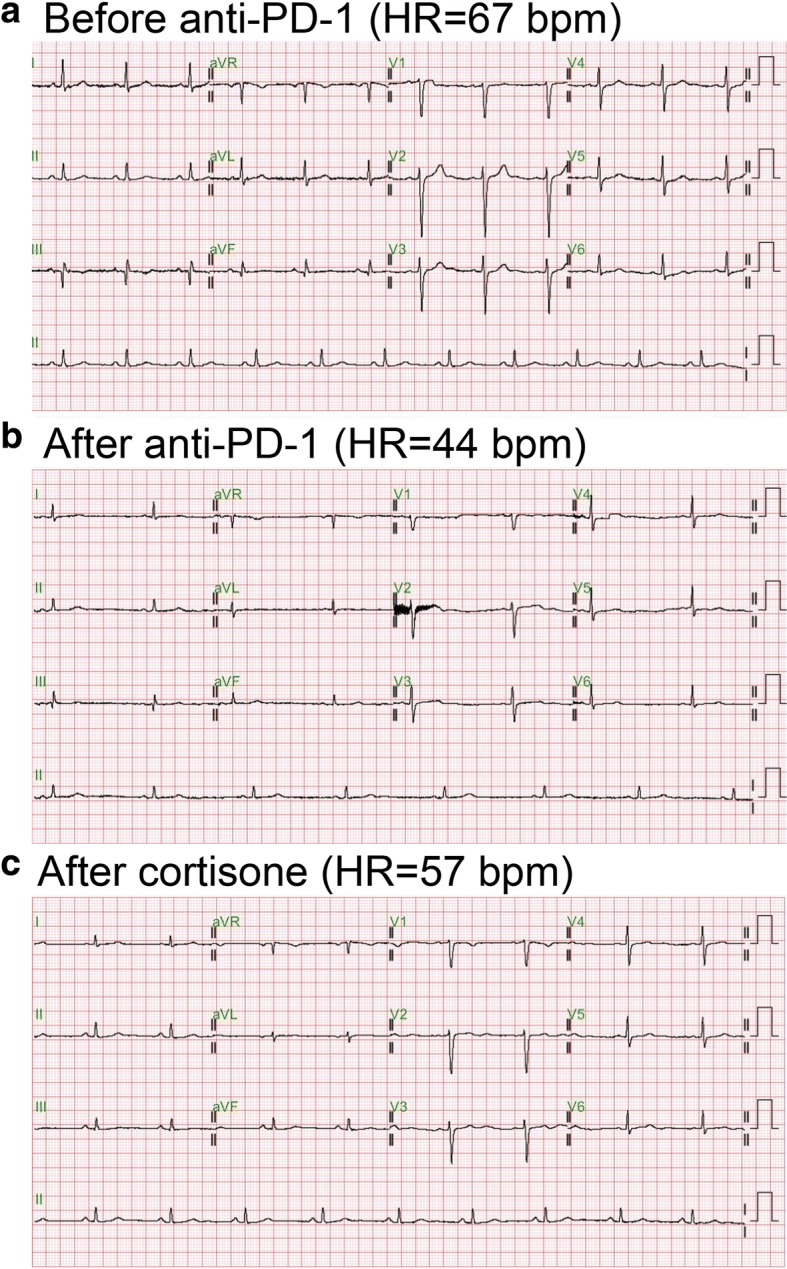
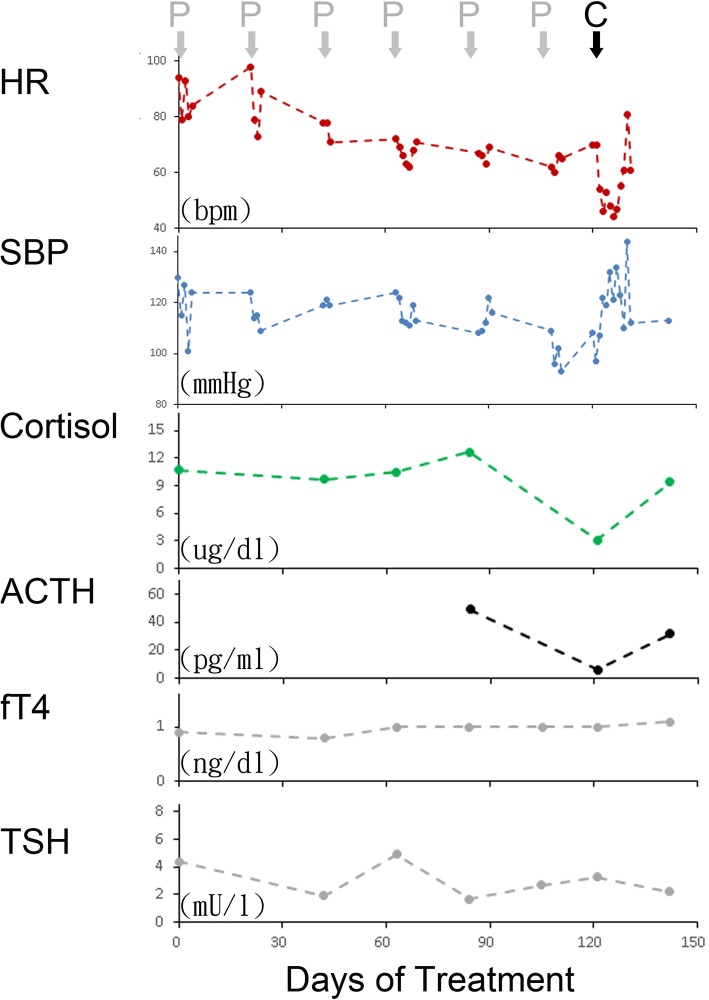
A 42-year-old male patient who had metastatic hepatocellular carcinoma failed treatment with sorafenib. Pembrolizumab at a fixed dose of 100 mg every three weeks was given. His heart rate gradually slowed down and he presented sick sinus syndrome with a lowest heart rate of 38 bpm after six cycles of pembrolizumab. He denied chest tightness, cold sweating, palpitation and dyspnea. Lab data including cardiac enzyme, electrolytes and thyroid function were all within a normal range. Simultaneously, he complained of fatigue, dizziness and anorexia with hypotension. Lab data revealed low cortisol and ACTH levels. Anti-PD-1 induced adrenal insufficiency was suspected. Low-dose cortisone (12.5 mg) was prescribed, and the patient's symptoms, hypotension and sick sinus syndrome showed rapid improvement. Cortisone was gradually titrated and discontinued three weeks later. His sick sinus syndrome did not relapse and the cortisol and ACTH level returned to normal.
Sick sinus syndrome caused by anti-PD-1 treatment is a rare adverse event. With the development of sick sinus syndrome, myocarditis should be the first differential diagnosis because of its lethality. From this case, we learned that sick sinus syndrome may be a presentation of immune- or adrenal insufficiency-mediated sinus node dysfunction, both could be reversed with a glucocorticoid supplement.
抗程序性细胞死亡蛋白-1(抗 PD-1)的应用已成功治疗多种癌症。尽管疗效显著,但免疫相关不良反应仍是一个主要关注点。免疫相关的心脏毒性虽然罕见但致命,最近已成为关注焦点。已报道包括心肌炎、心肌病、心脏纤维化、心脏传导阻滞和心脏骤停在内的心脏毒性。其中,心肌炎常伴有心律失常。作为免疫相关不良反应的病态窦房结综合征的表现尚未报道。在此,我们报告首例由抗 PD-1 引起的病态窦房结综合征,这是一种罕见的毒性。
一名 42 岁男性患者,患有转移性肝细胞癌,索拉非尼治疗失败。给予每 3 周固定剂量 100mg 的派姆单抗。他的心率逐渐减慢,在接受派姆单抗治疗 6 个周期后出现病态窦房结综合征,最低心率为 38bpm。他否认胸闷、冷汗、心悸和呼吸困难。包括心肌酶、电解质和甲状腺功能在内的实验室数据均在正常范围内。同时,他伴有疲劳、头晕和厌食症,并出现低血压。实验室数据显示皮质醇和 ACTH 水平较低。怀疑为抗 PD-1 诱导的肾上腺功能不全。给予小剂量可的松(12.5mg),患者的症状、低血压和病态窦房结综合征迅速改善。逐渐调整可的松剂量,3 周后停用。他的病态窦房结综合征未复发,皮质醇和 ACTH 水平恢复正常。
抗 PD-1 治疗引起的病态窦房结综合征是一种罕见的不良反应。随着病态窦房结综合征的发展,由于其致命性,心肌炎应作为首要鉴别诊断。从这个病例中,我们了解到病态窦房结综合征可能是免疫或肾上腺功能不全介导的窦房结功能障碍的表现,都可以通过补充糖皮质激素来逆转。