Gerhardt Attard, The Institute of Cancer Research and the Royal Marsden National Health Service Foundation Trust, London, United Kingdom; Michael Borre, Aarhus University Hospital, Aarhus, Denmark; Howard Gurney, Macquarie University, Sydney, New South Wales, Australia; Yohann Loriot, Gustave Roussy, Institut National de la Santé et de la Recherche Médicale U981, University of Paris Saclay, Villejuif, France; Corina Andresen-Daniil, Ranjith Kalleda, and Trinh Pham, Pfizer, New York, NY; and Mary-Ellen Taplin, Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA.
J Clin Oncol. 2018 Sep 1;36(25):2639-2646. doi: 10.1200/JCO.2018.77.9827. Epub 2018 Jul 20.
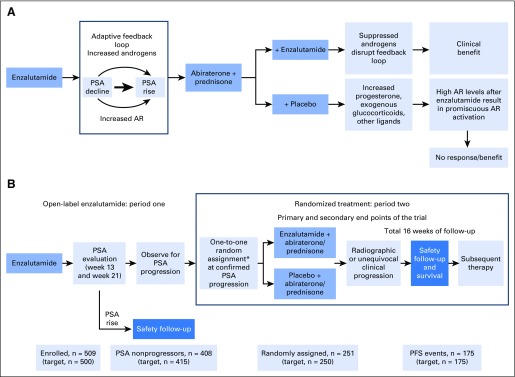
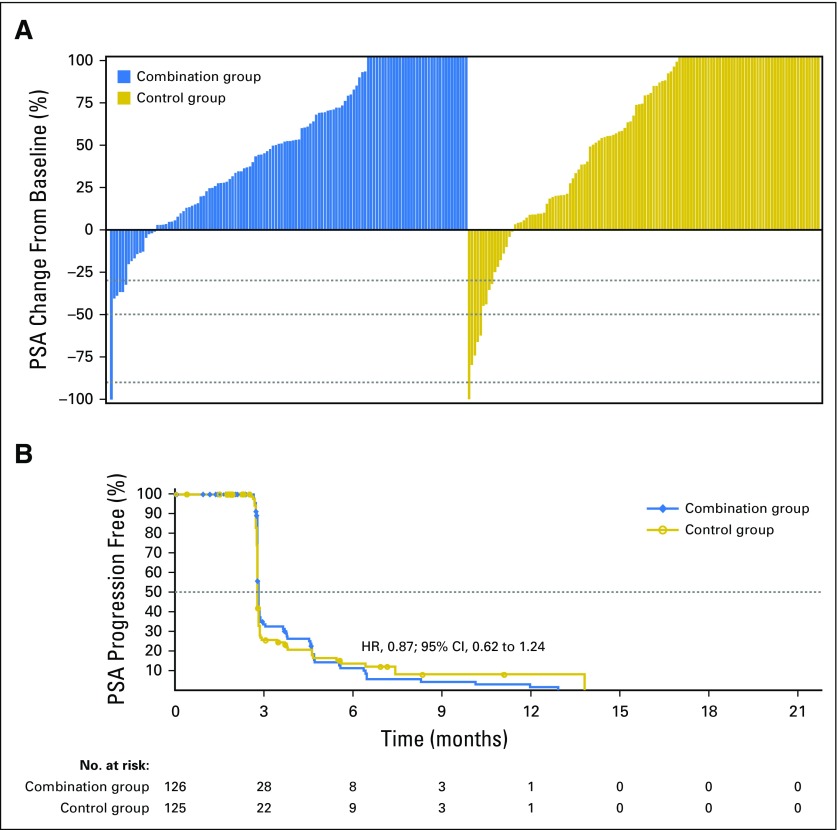
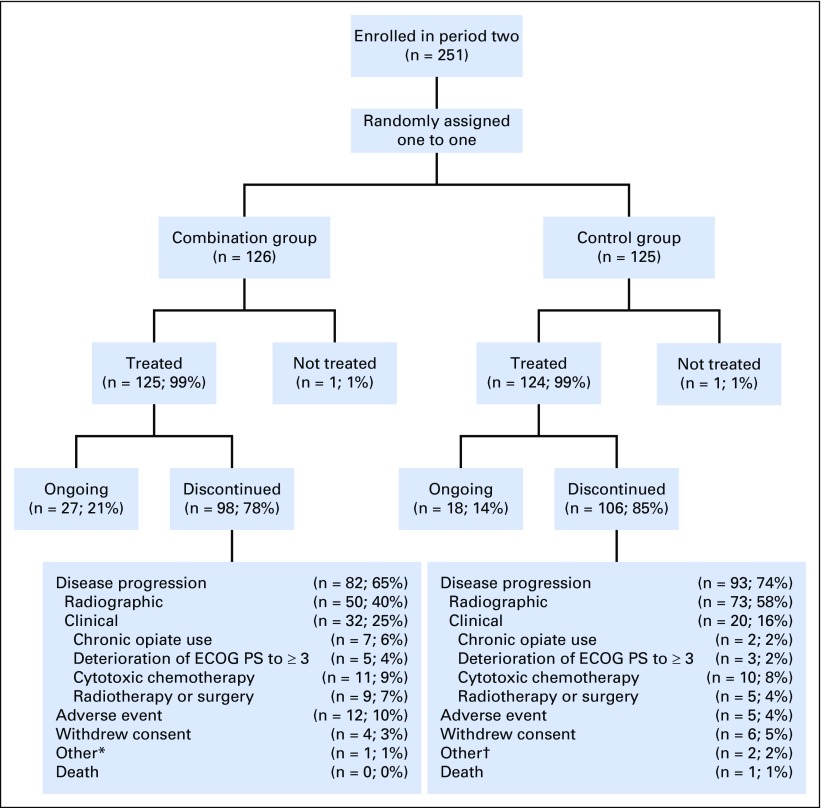
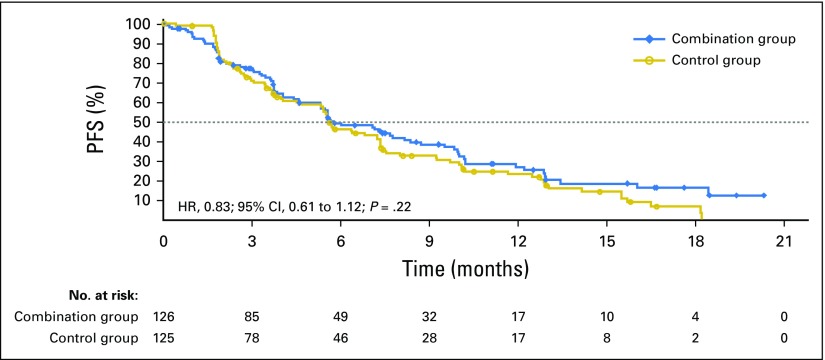
Purpose Enzalutamide resistance could result from raised androgens and be overcome by combination with abiraterone acetate. PLATO ( ClinicalTrials.gov identifier: NCT01995513) interrogated this hypothesis using a randomized, double-blind, placebo-controlled design. Patients and Methods In period one, men with chemotherapy-naïve metastatic castration-resistant prostate cancer received open-label enzalutamide 160 mg daily. Men with no prostate-specific antigen (PSA) increase at weeks 13 and 21 were treated until PSA progression (≥ 25% increase and ≥ 2 ng/mL above nadir), then randomly assigned at a one-to-one ratio in period two to abiraterone acetate 1,000 mg daily and prednisone 5 mg twice daily with either enzalutamide or placebo (combination or control group, respectively) until disease progression as defined by the primary end point: progression-free survival (radiographic or unequivocal clinical progression or death during study). Secondary end points included time to PSA progression and PSA response in period two. Results Of 509 patients enrolled in period one, 251 were randomly assigned in period two. Median progression-free survival was 5.7 months in the combination group and 5.6 months in the control group (hazard ratio, 0.83; 95% CI, 0.61 to 1.12; P = .22). There was no difference in the secondary end points. Grade 3 hypertension (10% v 2%) and increased ALT (6% v 2%) or AST (2% v 0%) were more frequent in the combination than the control group. Conclusion Combining enzalutamide with abiraterone acetate and prednisone is not indicated after PSA progression during treatment with enzalutamide alone; hypertension and elevated liver enzymes are more frequent with combination therapy.
雄激素升高可能导致恩扎鲁胺耐药,并可通过与醋酸阿比特龙联合治疗克服。PLATO(ClinicalTrials.gov 标识符:NCT01995513)采用随机、双盲、安慰剂对照设计检验了这一假说。
在第一阶段,未经化疗的转移性去势抵抗性前列腺癌患者接受开放标签的恩扎鲁胺 160mg 每日一次治疗。在第 13 周和第 21 周时前列腺特异性抗原(PSA)无增加的患者继续治疗,直至 PSA 进展(≥25%增加且≥2ng/ml 高于最低点),然后在第二阶段以 1:1 的比例随机分配至醋酸阿比特龙 1000mg 每日一次和泼尼松 5mg 每日两次,分别联合或不联合恩扎鲁胺治疗,直至主要终点定义的疾病进展:无进展生存期(影像学或明确临床进展或研究期间死亡)。次要终点包括第二阶段的 PSA 进展时间和 PSA 反应。
在第一阶段纳入的 509 例患者中,有 251 例患者被随机分配至第二阶段。联合组的中位无进展生存期为 5.7 个月,对照组为 5.6 个月(风险比,0.83;95%CI,0.61 至 1.12;P =.22)。次要终点无差异。联合组的 3 级高血压(10%比 2%)和 ALT(6%比 2%)或 AST(2%比 0%)升高更为常见。
在单独使用恩扎鲁胺治疗期间 PSA 进展后,联合恩扎鲁胺与醋酸阿比特龙和泼尼松治疗并不适用;联合治疗时高血压和肝酶升高更为常见。