Department of Anesthesiology and Pain Medicine, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
Institute for Research in Cardiac Anesthesia, Munich, Germany.
PLoS One. 2018 Aug 3;13(8):e0201647. doi: 10.1371/journal.pone.0201647. eCollection 2018.
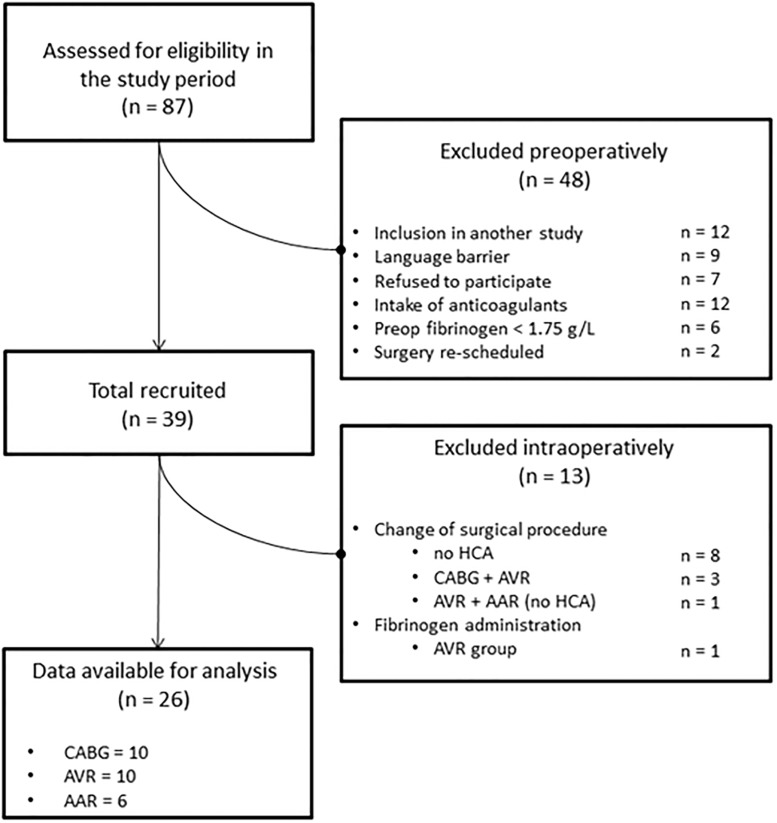
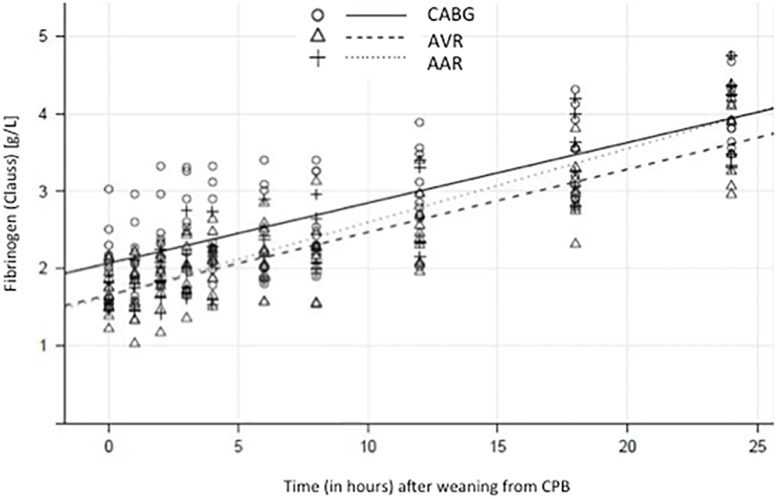
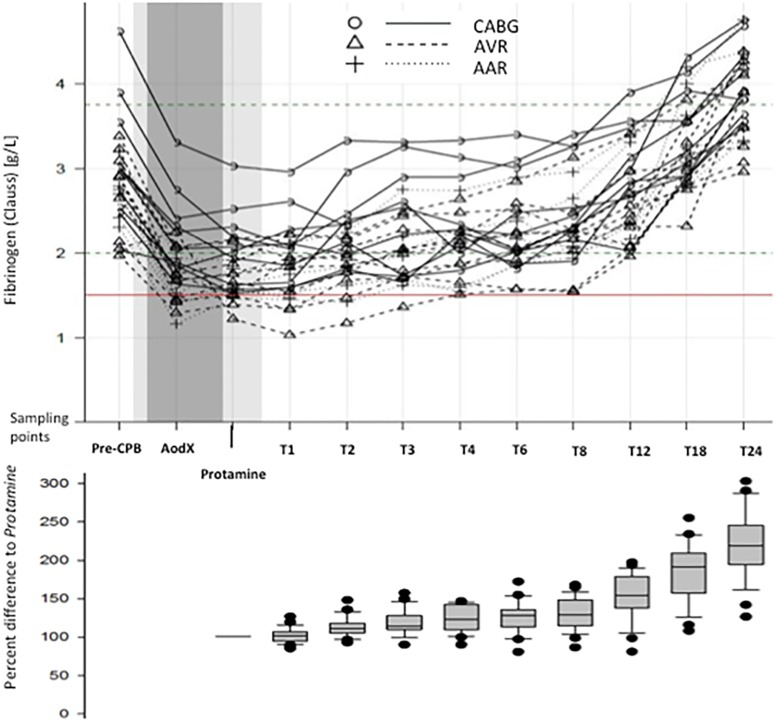
Low plasma fibrinogen level is common after cardiopulmonary bypass (CPB). Current substitution practice with fibrinogen concentrate generally follows a single measurement and cut-off values from the literature, whereas early postoperative endogenous fibrinogen kinetics is incompletely described and widely disregarded. The aim of this study was to determine the short-term recovery pattern of plasma fibrinogen after CPB weaning. Our hypothesis was that in the absence of surgical bleeding, CPB-induced hypofibrinogenemia would resolve spontaneously and predictably within a few hours. In a prospective, observational study of 26 patients undergoing conventional CPB (cCPB) or minimally invasive extracorporeal circulation (MiECC), Clauss fibrinogen level (C-FIB) was determined at 10 closely spaced time points after protamine administration. Primary endpoint was the time to recovery of post-CPB fibrinogen levels to ≥1.5 g/L. C-FIB reached its nadir after protamine administration corresponding to 62 ± 5% (mean ± SD) of the baseline level after cCPB and 68 ± 7% after MiECC (p = 0.027 vs. cCPB). C-FIB recovered spontaneously at a nearly constant rate of approximately 0.08 g/L per hour. In all patients, C-FIB was ≥1.5 g/L at 4 hours and ≥2.0 g/L at 13 hours after CPB weaning. Following cardiac surgery with CPB and in the absence of surgical bleeding, spontaneous recovery of normal endogenous fibrinogen levels can be expected at a rate of 0.08 g/L per hour. Administration of fibrinogen concentrate triggered solely by a single-point measurement of low plasma fibrinogen some time after CPB is not justified.
体外循环(CPB)后血浆纤维蛋白原水平降低较为常见。目前纤维蛋白原浓缩物的替代治疗通常根据文献中的单次测量和截断值来进行,而术后早期内源性纤维蛋白原动力学尚未完全描述,且未得到广泛重视。本研究旨在确定 CPB 脱机后血浆纤维蛋白原的短期恢复模式。我们的假设是,在没有手术出血的情况下,CPB 引起的低纤维蛋白原血症会在数小时内自发且可预测地得到解决。在一项对 26 例行常规体外循环(cCPB)或微创体外循环(MiECC)的患者进行的前瞻性、观察性研究中,在鱼精蛋白给药后 10 个时间点密切间隔测定 Clauss 纤维蛋白原水平(C-FIB)。主要终点是 CPB 后纤维蛋白原水平恢复至≥1.5 g/L 的时间。C-FIB 在鱼精蛋白给药后达到最低值,对应于 cCPB 后基础值的 62±5%(平均值±标准差)和 MiECC 后 68±7%(p=0.027 与 cCPB 相比)。C-FIB 以接近恒定的速度,即每小时约 0.08 g/L 自发恢复。在所有患者中,CPB 脱机后 4 小时时 C-FIB 均≥1.5 g/L,13 小时时 C-FIB 均≥2.0 g/L。在接受 CPB 心脏手术后,且无手术出血的情况下,可预计正常内源性纤维蛋白原水平以每小时 0.08 g/L 的速度自发恢复。在 CPB 后某个时间点根据单次低血浆纤维蛋白原测量值来触发纤维蛋白原浓缩物的给药是不合理的。