VA Center for Clinical Management Research, VA Ann Arbor Healthcare System, Ann Arbor, Michigan, USA.
Department of Internal Medicine, University of Michigan Medical School, Ann Arbor, Michigan, USA.
BMJ Qual Saf. 2019 Jan;28(1):56-66. doi: 10.1136/bmjqs-2018-008025. Epub 2018 Aug 12.
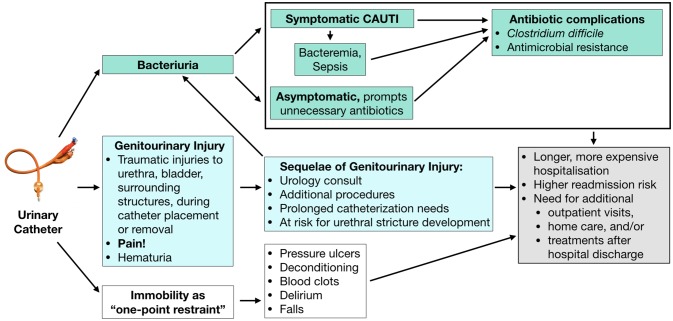
Indwelling urinary catheters are commonly used for patients undergoing general and orthopaedic surgery. Despite infectious and non-infectious harms of urinary catheters, there is limited guidance available to surgery teams regarding appropriate perioperative catheter use.
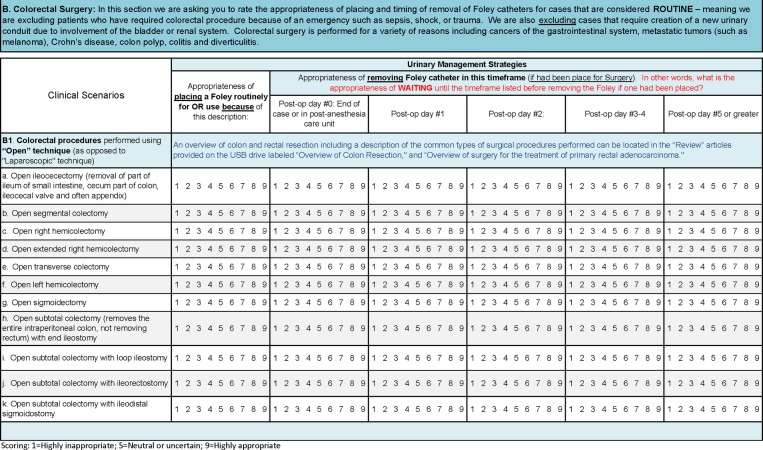
Using the RAND Corporation/University of California Los Angeles (RAND/UCLA) Appropriateness Method, we assessed the appropriateness of indwelling urinary catheter placement and different timings of catheter removal for routine general and orthopaedic surgery procedures.
Two multidisciplinary panels consisting of 13 and 11 members (physicians and nurses) for general and orthopaedic surgery, respectively, reviewed the available literature regarding the impact of different perioperative catheter use strategies. Using a standardised, multiround rating process, the panels independently rated clinical scenarios (91 general surgery, 36 orthopaedic surgery) for urinary catheter placement and postoperative duration of use as appropriate (ie, benefits outweigh risks), inappropriate or of uncertain appropriateness.
Appropriateness of catheter use varied by procedure, accounting for procedure-specific risks as well as expected procedure time and intravenous fluids. Procedural appropriateness ratings for catheters were summarised for clinical use into three groups: (1) can perform surgery without catheter; (2) use intraoperatively only, ideally remove before leaving the operating room; and (3) use intraoperatively and keep catheter until postoperative days 1-4. Specific recommendations were provided by procedure, with postoperative day 1 being appropriate for catheter removal for first voiding trial for many procedures.
We defined the appropriateness of indwelling urinary catheter use during and after common general and orthopaedic surgical procedures. These ratings may help reduce catheter-associated complications for patients undergoing these procedures.
在接受普通外科和骨科手术的患者中,留置导尿管通常被用于导尿。尽管导尿管存在感染和非感染危害,但针对手术团队在围手术期使用导尿管的问题,目前提供的指导有限。
我们使用 RAND 公司/加州大学洛杉矶分校(RAND/UCLA)适宜性方法,评估了留置导尿管放置的适宜性,以及不同的导尿管拔除时机在常规普通外科和骨科手术中的应用。
两个多学科小组分别由 13 名和 11 名成员(医生和护士)组成,分别负责普通外科和骨科手术。这两个小组审查了关于不同围手术期导尿管使用策略影响的现有文献。使用标准化的多轮评分过程,小组独立对临床情况(91 例普通外科,36 例骨科手术)进行了评分,评估导尿管放置和术后使用时间的适宜性(即,获益超过风险)、不适宜或适宜性不确定。
导尿管使用的适宜性因手术而异,考虑到了特定手术的风险以及预期手术时间和静脉输液量。手术过程中对导尿管使用的适宜性评分进行了总结,为临床应用分为三组:(1)可以在没有导尿管的情况下进行手术;(2)仅在手术期间使用,理想情况下在离开手术室之前移除;(3)在手术期间和术后第 1-4 天使用。根据具体的手术程序提供了具体的建议,对于许多手术,术后第 1 天适合用于首次排尿试验时拔除导尿管。
我们确定了在普通外科和骨科手术中留置导尿管的适宜性。这些评分可能有助于减少接受这些手术的患者的导尿管相关并发症。