Tanimura Akira, Hirai Risen, Nakamura Miki, Takeshita Masataka, Hagiwara Shotaro, Miwa Akiyoshi
Department of Hematology, Tokyo-Kita Medical Center, Japan.
Division of Hematology, National Center for Global Health and Medicine, Japan.
Intern Med. 2018 Dec 15;57(24):3521-3528. doi: 10.2169/internalmedicine.0990-18. Epub 2018 Aug 10.
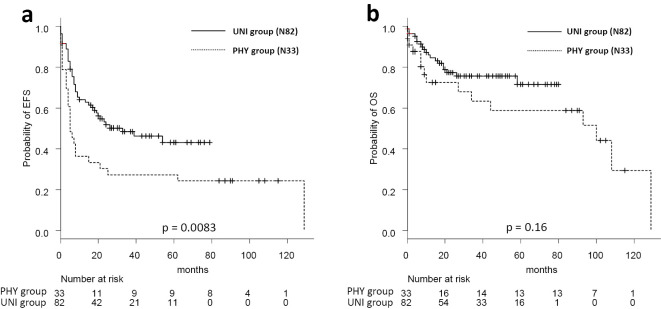
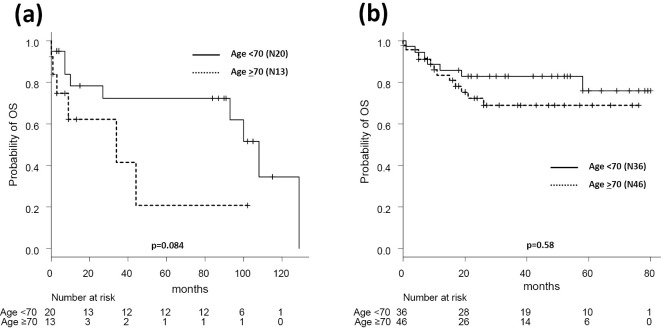
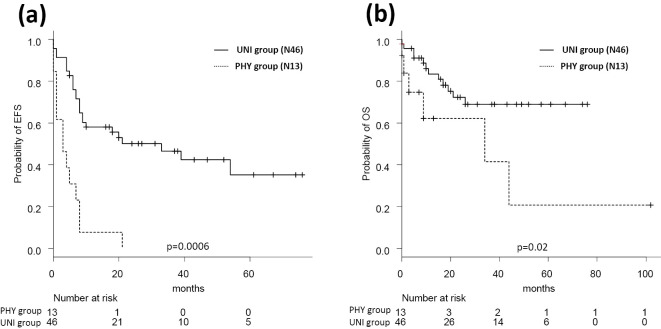
Objective Although R-CHOP (rituximab, cyclophosphamide, vincristine, doxorubicin, and prednisone) is a standard therapy for diffuse large B-cell lymphoma (DLBCL), the optimal dose for elderly patients remains unclear. Methods and Patients We retrospectively verified our R-CHOP dose-attenuation system implemented from 2005 for DLBCL patients. Among the 115 DLBCL patients treated during 2001-2010, 33 patients treated during 2001-2005 received R-CHOP doses adjusted according to physicians' decisions (PHY group). Eighty-two patients treated after 2005 received adjusted R-CHOP doses according to a unified dose-attenuation system (UNI group). Patients aged <60, 60-69, 70-79, and ≥80 years received the standard R-CHOP, 100% R-CHO+P (50 mg/m), 100% R+75% CHO+P (40 mg/m), and 100% R+50% CHO+P (30 mg/m), respectively. We compared the responses, survival, and treatment cessation between the PHY and UNI groups. Results The patients' characteristics between both groups were closely comparable. All PHY patients received randomly adjusted R-CHOP doses; 94% of UNI patients received scheduled doses. The complete response rates differed significantly between the UNI (77%) and PHY patients (50%) (p=0.011). The two-year event-free survival rates were 50% and 32% in the UNI and PHY groups, respectively (p=0.0083). The two-year OS rates were 77% and 72% in the UNI and PHY group (p=0.16). Among the patients aged >70 years (n=59) overall survival was shorter in the PHY group (62%) than in the UNI group (72%; p=0.02). The UNI group received higher anti-tumor agent doses than the PHY group. The therapy discontinuation rates were 5% in the UNI group and 24% in the PHY group. Conclusion Carrying out unified dose reduction may improve the efficacy and prognosis among elderly DLBCL patients.
目的 尽管利妥昔单抗、环磷酰胺、长春新碱、多柔比星和泼尼松(R-CHOP)是弥漫性大B细胞淋巴瘤(DLBCL)的标准疗法,但老年患者的最佳剂量仍不明确。方法与患者 我们回顾性验证了自2005年起实施的针对DLBCL患者的R-CHOP剂量调整系统。在2001年至2010年期间接受治疗的115例DLBCL患者中,2001年至2005年期间接受治疗的33例患者根据医生的决定接受调整后的R-CHOP剂量(PHY组)。2005年后接受治疗的82例患者根据统一的剂量调整系统接受调整后的R-CHOP剂量(UNI组)。年龄<60岁、60至69岁、70至79岁和≥80岁的患者分别接受标准R-CHOP、100%R-CHO+P(50mg/m²)、100%R+75%CHO+P(40mg/m²)和100%R+50%CHO+P(30mg/m²)。我们比较了PHY组和UNI组之间的反应、生存率和治疗中断情况。结果 两组患者的特征密切可比。所有PHY组患者均接受随机调整的R-CHOP剂量;94%的UNI组患者接受预定剂量。UNI组(77%)和PHY组患者(50%)的完全缓解率差异显著(p=0.011)。UNI组和PHY组的两年无事件生存率分别为50%和32%(p=0.0083)。UNI组和PHY组的两年总生存率分别为77%和72%(p=0.16)。在年龄>70岁的患者(n=59)中,PHY组的总生存率(62%)低于UNI组(72%;p=0.02)。UNI组接受的抗肿瘤药物剂量高于PHY组。UNI组的治疗中断率为5%,PHY组为24%。结论 进行统一的剂量降低可能会改善老年DLBCL患者的疗效和预后。