Department of Urology, Western General Hospital, Edinburgh, UK.
College of Medicine and Veterinary Medicine, University of Edinburgh, Edinburgh, UK.
BJU Int. 2019 Mar;123(3):429-438. doi: 10.1111/bju.14513. Epub 2018 Oct 9.
To report outcomes from a multiparametric (mp) magnetic resonance imaging (MRI)-based active surveillance programme that did not include performing protocol biopsies after the first confirmatory biopsy.
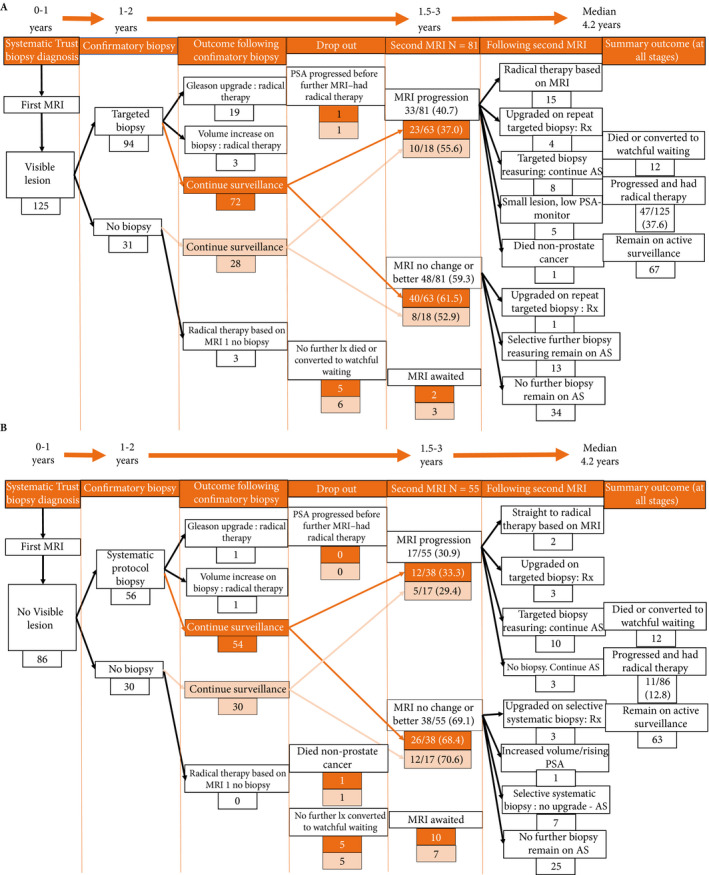
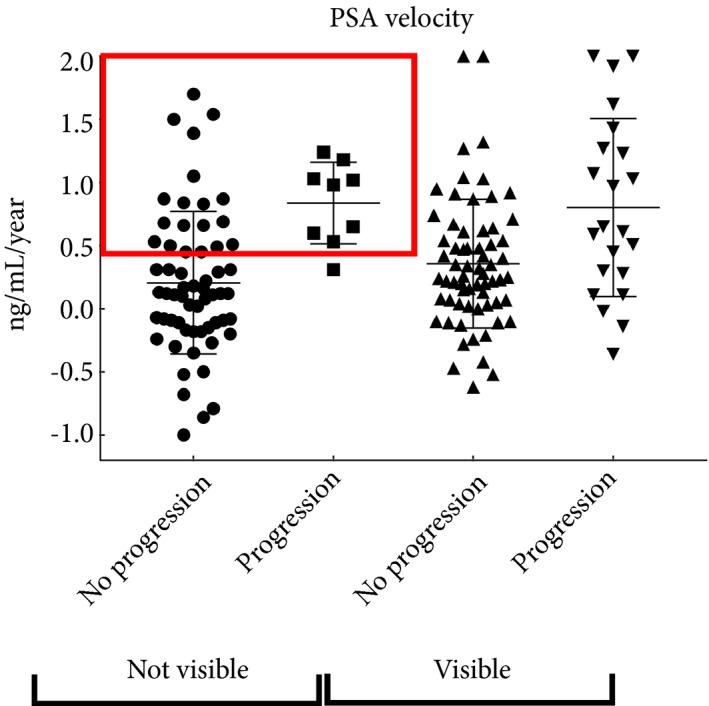
All patients diagnosed with Gleason 3 + 3 prostate cancer because of a raised PSA level who underwent mpMRI after diagnosis were included. Patients were recorded in a prospective clinical database and followed up with PSA monitoring and repeat MRI. In patients who remained on active surveillance after the first MRI (with or without confirmatory biopsy), we investigated PSA dynamics for association with subsequent progression. Comparison between first and second MRI scans was undertaken. Outcomes assessed were: progression to radical therapy at first MRI/confirmatory biopsy and progression to radical therapy in those who remained on active surveillance after first MRI.
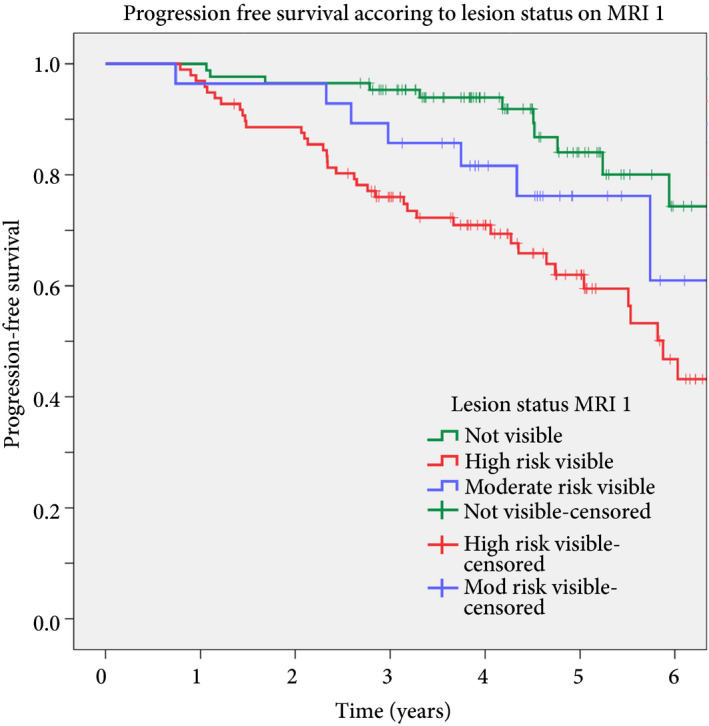
A total of 211 patients were included, with a median of 4.2 years of follow-up. The rate of progression to radical therapy was significantly greater at all stages among patients with visible lesions than in those with initially negative MRI (47/125 (37.6%) vs 11/86 (12.8%); odds ratio 4.1 (95% CI 2.0-8.5), P < 0.001). Only 1/56 patients (1.8%) with negative initial MRI scans who underwent a confirmatory systematic biopsy had upgrading to Gleason 3 + 4 disease. PSA velocity was significantly associated with subsequent progression in patients with negative initial MRI (area under the curve 0.85 [95% CI 0.75-0.94]; P <0.001). Patients with high-risk visible lesions on first MRI who remained on active surveillance had a high risk of subsequent progression 19/76 (25.0%) vs 9/84 (10.7%) for patients with no visible lesions, despite reassuring targeted and systematic confirmatory biopsies and regardless of PSA dynamics.
Men with low-risk Gleason 3 + 3 prostate cancer on active surveillance can forgo protocol biopsies in favour of MRI and PSA monitoring with selective re-biopsy.
报告一种多参数(mp)磁共振成像(MRI)主动监测方案的结果,该方案不包括在首次确认性活检后进行方案活检。
所有因 PSA 水平升高而被诊断为 Gleason 3+3 前列腺癌并在诊断后接受 mpMRI 的患者均被纳入研究。患者被记录在一个前瞻性临床数据库中,并通过 PSA 监测和重复 MRI 进行随访。在首次 MRI(有或无确认性活检)后仍接受主动监测的患者中,我们研究了 PSA 动力学与随后进展的关系。对首次和第二次 MRI 扫描进行了比较。评估的结果包括:首次 MRI/确认性活检时进展为根治性治疗以及首次 MRI 后仍接受主动监测的患者进展为根治性治疗。
共纳入 211 例患者,中位随访时间为 4.2 年。与初始 MRI 阴性的患者相比,有可见病变的患者进展为根治性治疗的比例在所有阶段均显著更高(47/125 [37.6%] vs 11/86 [12.8%];优势比 4.1 [95%CI 2.0-8.5],P<0.001)。仅 1/56(1.8%)初始 MRI 扫描阴性且接受系统确认性活检的患者升级为 Gleason 3+4 疾病。初始 MRI 阴性的患者中,PSA 速度与随后的进展显著相关(曲线下面积 0.85 [95%CI 0.75-0.94];P<0.001)。尽管进行了有针对性的和系统的确认性活检,并且 PSA 动力学也无变化,但首次 MRI 上有高危可见病变且仍接受主动监测的患者,其随后进展的风险很高(19/76 [25.0%] vs 9/84 [10.7%],无可见病变)。
在主动监测中,低危 Gleason 3+3 前列腺癌患者可以选择放弃方案活检,转而进行 MRI 和 PSA 监测,并选择性进行再活检。