Hansson-Hedblom Amanda, Almond Chrissy, Borgström Fredrik, Sly Indeg, Enkusson Dana, Troelsgaard Buchholt Anders, Karlsson Linda
Quantify Research AB, Stockholm, Sweden.
2BresMed, Sheffield, UK.
Cost Eff Resour Alloc. 2018 Aug 2;16:28. doi: 10.1186/s12962-018-0114-y. eCollection 2018.
Human monoclonal antibody ustekinumab is a novel Crohn's disease (CD) treatment blocking pro-inflammatory cytokines interleukin-12 and 23. The study's objective was to assess cost-effectiveness of ustekinumab in moderate to severely active CD in Sweden.
A cost-effectiveness model with an induction phase decision-tree structure and a maintenance phase Markov cohort structure was constructed. CD was represented by five health-states: remission, mild, moderate-severe, surgery and death. Ustekinumab was compared to adalimumab in patients who had failed conventional care, some of which had tried TNF-alpha-inhibitor(s) without experiencing treatment failure or side effects ("conventional care failure population") and to vedolizumab in patients previously failing TNF-alpha-inhibitor treatment. Discontinuation probabilities, utilities and ustekinumab induction efficacy were sourced from phase-III trials. Maintenance and comparator efficacy came from network-meta and treatment-sequence analyses. Resource use and unit costs were derived from literature and validated by clinical experts. The analysis had a societal perspective, a life-time time-horizon, and 2-year treatment duration. The results robustness was tested in univariate and probabilistic sensitivity analyses. Cost-effectiveness was estimated using quality-adjusted life-years (QALYs).
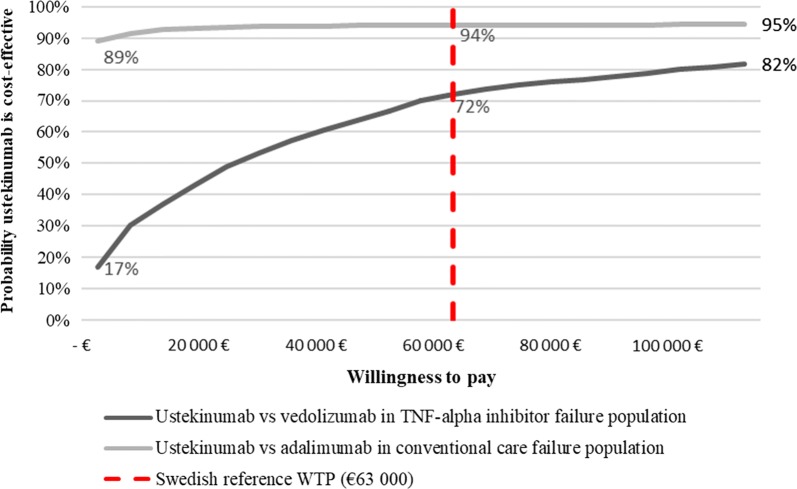
Ustekinumab dominated adalimumab in conventional care failure population (costs: - €6984, QALYs: + 0.232). In TNF-alpha-inhibitor failure population ustekinumab accrued 0.133 more QALYs than vedolizumab, yielding a €30,282 incremental cost-effectiveness ratio. Results were sensitive to decreasing the time horizon and increased treatment duration. At Swedish reference willingness-to-pay of €63,000 (SEK 600,000), ustekinumab had 94% probability of being cost-effective versus adalimumab, and 72% versus vedolizumab.
Results indicate ustekinumab dominates adalimumab in conventional care failure population, and is cost-effective versus vedolizumab in TNF-alpha-inhibitor failure population.
人源单克隆抗体优特克单抗是一种新型的克罗恩病(CD)治疗药物,可阻断促炎性细胞因子白细胞介素-12和23。本研究的目的是评估优特克单抗在瑞典中重度活动性CD患者中的成本效益。
构建了一个具有诱导期决策树结构和维持期马尔可夫队列结构的成本效益模型。CD由五个健康状态表示:缓解、轻度、中重度、手术和死亡。将优特克单抗与传统治疗失败的患者中的阿达木单抗进行比较,其中一些患者曾尝试使用肿瘤坏死因子-α抑制剂但未出现治疗失败或副作用(“传统治疗失败人群”),并与先前使用肿瘤坏死因子-α抑制剂治疗失败的患者中的维多珠单抗进行比较。停药概率、效用和优特克单抗诱导疗效来自III期试验。维持期和对照疗效来自网络荟萃分析和治疗序列分析。资源使用和单位成本来自文献并经临床专家验证。该分析采用社会视角、终身时间范围和2年治疗持续时间。在单变量和概率敏感性分析中测试了结果的稳健性。使用质量调整生命年(QALY)评估成本效益。
在传统治疗失败人群中,优特克单抗优于阿达木单抗(成本:-6984欧元,QALY:+0.232)。在肿瘤坏死因子-α抑制剂治疗失败人群中,优特克单抗比维多珠单抗多获得0.133个QALY,产生30282欧元的增量成本效益比。结果对缩短时间范围和延长治疗持续时间敏感。按照瑞典63000欧元(600000瑞典克朗)的参考支付意愿,优特克单抗与阿达木单抗相比具有成本效益的概率为94%,与维多珠单抗相比为72%。
结果表明,在传统治疗失败人群中,优特克单抗优于阿达木单抗,在肿瘤坏死因子-α抑制剂治疗失败人群中,与维多珠单抗相比具有成本效益。