Clinical Pharmacology and Pharmacometrics, AbbVie Deutschland GmbH & Co. KG, Ludwigshafen am Rhein, Germany.
Clinical Pharmacology and Pharmacometrics, AbbVie Inc., 1 North Waukegan Road, North Chicago, IL, 60064, USA.
Clin Pharmacokinet. 2019 Mar;58(3):375-387. doi: 10.1007/s40262-018-0704-z.
Risankizumab is a humanized anti-interleukin-23 monoclonal antibody in development for the treatment of several inflammatory diseases. This work characterized the pharmacokinetics of risankizumab and evaluated covariates that may affect its exposures using phase I and II trial data in subjects with psoriasis and Crohn's disease.
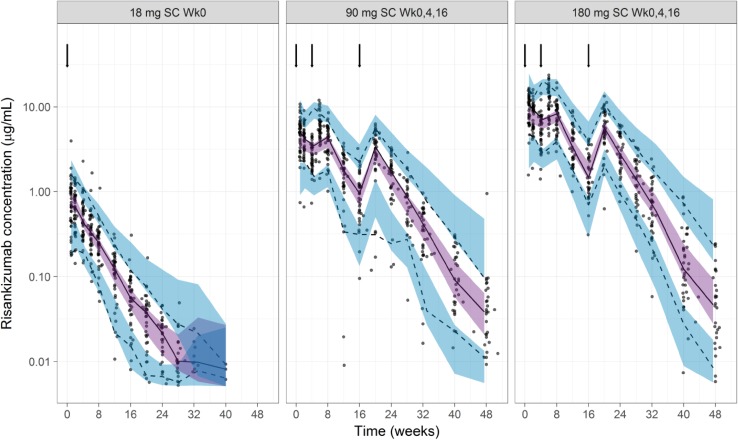
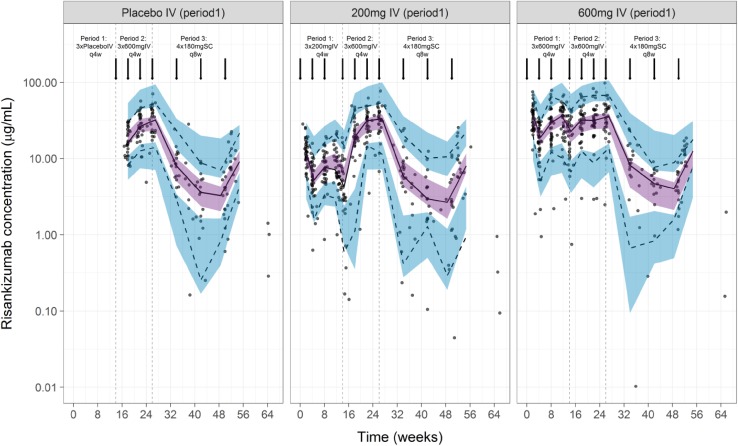
Plasma concentration measurements from a phase I study and a phase II study in subjects with psoriasis (n = 157; single doses of 0.01-5 mg/kg intravenously, 0.25-1 mg/kg subcutaneously, and 18 mg subcutaneously, and multiple doses of 90 and 180 mg subcutaneously), and a phase II study in subjects with Crohn's disease (n = 115; doses of 200 or 600 mg intravenously every 4 weeks followed by 180 mg subcutaneously every 8 weeks) were analyzed using non-linear mixed-effects modeling. The model was qualified using bootstrap and simulation-based diagnostics.
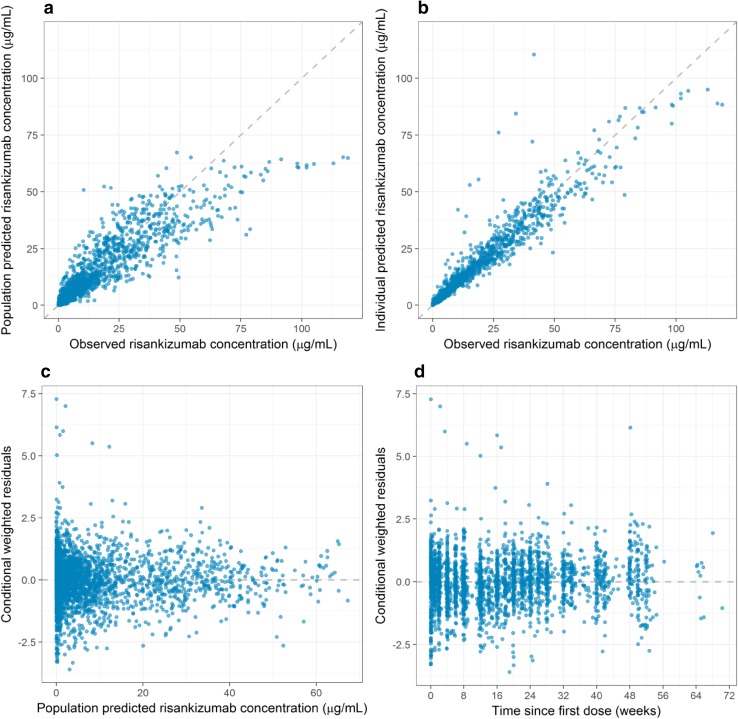
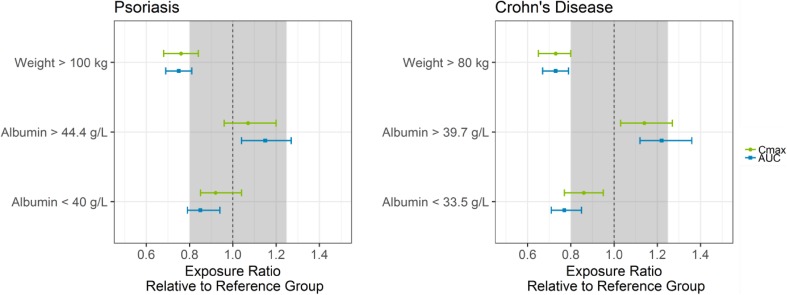
A two-compartment model with first-order absorption and elimination described the pharmacokinetics of risankizumab. Considering the body weight and baseline albumin central tendency differences between disease populations, risankizumab clearance, steady-state volume of distribution, and terminal-phase elimination half-life were estimated to be approximately 0.35 L/day, 11.7 L, and 27 days, respectively, for a typical 90-kg subject with psoriasis with an albumin level of 42 g/L, and 0.31 L/day, 8.45 L, and 22 days, respectively, for a typical 65-kg subject with Crohn's disease with an albumin level of 37 g/L. Risankizumab absolute subcutaneous bioavailability and absorption rate constant were 72% and 0.18 day, respectively. Inter-individual variability for clearance was 37%.
Risankizumab displayed pharmacokinetic characteristics typical for an IgG1 monoclonal antibody with no apparent target-mediated disposition. Accounting for the effects of body weight and baseline albumin explained the small differences in the pharmacokinetics of risankizumab between psoriasis and Crohn's disease, with no further differences between the patient populations.
risankizumab 是一种人源化抗白细胞介素-23 单克隆抗体,目前正在开发用于治疗多种炎症性疾病。本研究采用来自银屑病和克罗恩病患者的 I 期和 II 期临床试验数据,对 risankizumab 的药代动力学特征进行了描述,并评估了可能影响其暴露量的协变量。
对来自银屑病 I 期研究(n=157;静脉注射 0.01-5mg/kg、皮下注射 0.25-1mg/kg 和皮下注射 18mg,以及皮下注射 90 和 180mg 多次给药)和 II 期研究(n=115;静脉注射 200 或 600mg,每 4 周 1 次,随后皮下注射 180mg,每 8 周 1 次)的受试者的血浆浓度进行了非线性混合效应模型分析。采用 bootstrap 和基于模拟的诊断方法对模型进行了验证。
risankizumab 的药代动力学采用具有一级吸收和消除的两室模型进行描述。考虑到疾病人群之间的体重和基线白蛋白中心趋势差异,估计对于体重为 90kg、白蛋白水平为 42g/L 的典型银屑病患者,risankizumab 的清除率、稳态分布容积和终末消除半衰期分别约为 0.35L/天、11.7L 和 27 天;对于体重为 65kg、白蛋白水平为 37g/L 的典型克罗恩病患者,risankizumab 的清除率、稳态分布容积和终末消除半衰期分别约为 0.31L/天、8.45L 和 22 天。risankizumab 的绝对皮下生物利用度和吸收速率常数分别为 72%和 0.18 天。清除的个体间变异性为 37%。
risankizumab 表现出与 IgG1 单克隆抗体典型的药代动力学特征,不存在明显的靶向介导处置。考虑到体重和基线白蛋白的影响,可以解释 risankizumab 在银屑病和克罗恩病之间的药代动力学差异较小,而在患者人群中没有进一步的差异。