PATH, PO Box 900922, Seattle, WA 98109, USA.
Makerere University, College of Health Sciences, School of Public Health, PO Box 7072, Kampala, Uganda.
Contraception. 2018 Nov;98(5):423-429. doi: 10.1016/j.contraception.2018.08.007. Epub 2018 Aug 17.
The aim of this study was to examine continuation of subcutaneous and intramuscular depot medroxyprogesterone acetate (DMPA-SC and DMPA-IM) when administered by facility-based health workers in Burkina Faso and Village Health Teams (VHTs) in Uganda.
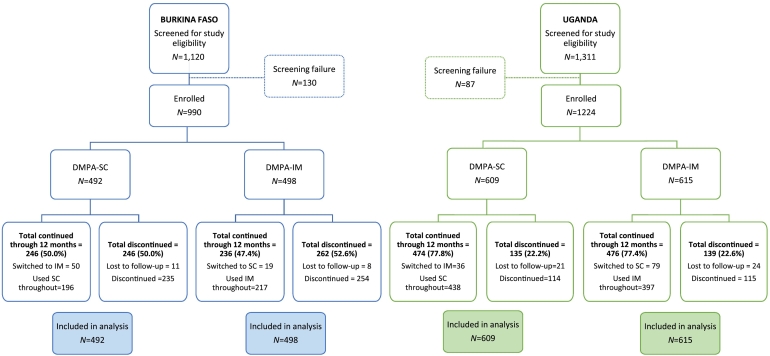
Participants were family planning clients of health centers (Burkina Faso) or VHTs (Uganda) who had decided to initiate injectable use. Women selected DMPA-SC or DMPA-IM and study staff followed them for up to four injections (providing 12 months of pregnancy protection) to determine contraceptive continuation. Study staff interviewed women at their first injection (baseline), second injection, fourth injection and if they discontinued either product.
Twelve-month continuation in Burkina Faso was 50% for DMPA-SC and 47.4% for DMPA-IM (p=.41, N=990, 492 DMPA-SC and 498 DMPA-IM). Twelve-month continuation in Uganda was 77.8% for DMPA-SC and 77.4% for DMPA-IM (p=.85, N=1224, 609 DMPA-SC and 615 DMPA-IM). Reasons for discontinuation of DMPA across groups in Burkina Faso included side effects (90/492, 18.3%), being late for injection (68/492, 13.8%) and refusal of spouse (51/492, 10.4%). Reasons for discontinuation in Uganda included being late for injection (65/229, 28.4%), received from non-VHT (50/229, 21.8%) and side effects (34/229, 14.8%). Increased age (adjusted hazard ratio=0.98, p=.01) and partner acceptance of family planning (adjusted hazard ratio=0.48, p<.001) had protective effects against discontinuation in Burkina Faso; we did not find statistically significant variables in Uganda.
There is no difference in 12-month continuation (through four injections) between DMPA-SC and DMPA-IM whether from facility-based health workers in Burkina Faso or VHTs in Uganda. Continuation was higher through community-based distribution in Uganda than health facilities in Burkina Faso.
The subcutaneous formulation of depot medroxyprogesterone acetate (DMPA-SC) is increasingly available in Family Planning 2020 countries. Use of DMPA-SC does not appear to change continuation relative to traditional intramuscular DMPA. Growing evidence of DMPA-SC's suitability for community-based distribution and self-injection may yield indirect benefits for contraceptive continuation and help reach new users.
本研究旨在考察在布基纳法索的医疗机构工作人员和乌干达的乡村卫生团队中,皮下和肌肉内注射长效醋酸甲羟孕酮(DMPA-SC 和 DMPA-IM)的续用情况。
参与者为布基纳法索卫生中心的计划生育客户或乌干达的乡村卫生团队的计划生育客户,他们决定开始使用注射避孕。女性选择 DMPA-SC 或 DMPA-IM,研究人员为她们提供最多 4 次注射(提供 12 个月的妊娠保护),以确定避孕的续用情况。研究人员在女性首次注射(基线)、第二次注射、第四次注射时对其进行访谈,如果她们停止使用任何一种产品也会进行访谈。
布基纳法索的 12 个月续用率为 DMPA-SC 组 50%,DMPA-IM 组 47.4%(p=.41,N=990,492 例 DMPA-SC 和 498 例 DMPA-IM)。乌干达的 12 个月续用率为 DMPA-SC 组 77.8%,DMPA-IM 组 77.4%(p=.85,N=1224,609 例 DMPA-SC 和 615 例 DMPA-IM)。布基纳法索 DMPA 停药的原因包括副作用(90/492,18.3%)、错过注射时间(68/492,13.8%)和配偶拒绝(51/492,10.4%)。乌干达停药的原因包括错过注射时间(65/229,28.4%)、非 VHT 提供(50/229,21.8%)和副作用(34/229,14.8%)。年龄较大(调整后的风险比=0.98,p=.01)和伴侣接受计划生育(调整后的风险比=0.48,p<.001)对布基纳法索的停药具有保护作用;我们在乌干达没有发现具有统计学意义的变量。
在布基纳法索由医疗机构工作人员或乌干达的乡村卫生团队提供的 DMPA-SC 和 DMPA-IM,12 个月的续用率(通过 4 次注射)没有差异。在乌干达,通过社区为基础的分发方式,DMPA 的续用率高于布基纳法索的卫生机构。
在计划生育 2020 年国家中,长效醋酸甲羟孕酮(DMPA-SC)的皮下制剂越来越普及。与传统的肌肉内注射 DMPA 相比,DMPA-SC 的使用似乎不会改变续用率。DMPA-SC 适合社区为基础的分发和自我注射的证据越来越多,可能会对避孕的续用产生间接影响,并有助于接触新的使用者。