Department of Neurosurgery, Universitair Ziekenhuis Brussel, Brussels, Belgium.
Department of Medical Oncology, Universitair Ziekenhuis Brussel, Brussels, Belgium.
Cancer Med. 2018 Oct;7(10):4870-4879. doi: 10.1002/cam4.1726. Epub 2018 Aug 21.
Up to 60% of patients with metastatic melanoma develop melanoma brain metastasis (MBM) during the course of their disease. Surgery, radiosurgery (SRS), stereotactic radiotherapy (SRT), and whole-brain radiation therapy (WBRT) or combinations of these are commonly used local treatment modalities. Inhibitory monoclonal antibodies against the CTLA-4 and PD-1 immune checkpoint receptors significantly improved the survival of metastatic melanoma patients, including patients with MBM. This prolonged survival, and potentially also the immunostimulatory mechanisms, may expose patients to a higher risk for long-term complications such as focal postradiation necrosis of the brain (RNB).
We analyzed the incidence of pseudotumoral RNB in a single institution cohort of 142 melanoma patients that were prospectively followed after starting treatment with pembrolizumab in an expanded access program.
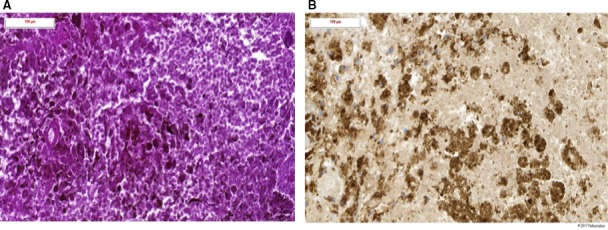
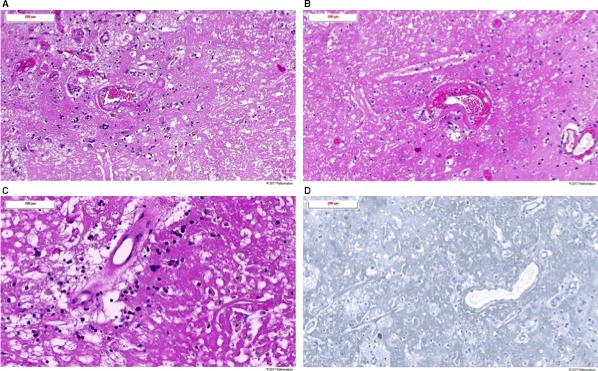
Of the 142 patients, 43 (30.7%) patients had MBM at initiation pembrolizumab. Of these, 31 (72.1%) were treated with SRS, 8 (18.6%) with WBRT while 4 (9.3%) had no prior local therapy. Of patients treated with RT, 28 (71.1%) received RT before the initiation of pembrolizumab. 5 (12.8%) patients developed a new symptomatic pseudotumoral lesion at a median time of 11.15 months (range 8-46) after the RT. In all patients, the diagnosis of RNB was radiologically confirmed. The RNB was treated with corticosteroids in two patients, bevacizumab in two patients, and surgery in three symptomatic patients. The diagnosis was histologically confirmed in the patients treated with surgery.
Melanoma patients with MBM treated with radiosurgery and showing a beneficial response to pembrolizumab are at risk for late RNB. In case of suspected isolated progression at the site of a previously irradiated MBM, the diagnosis of RNB should be considered.
在疾病过程中,多达 60%的转移性黑色素瘤患者会发展为黑色素瘤脑转移(MBM)。手术、放射外科手术(SRS)、立体定向放射治疗(SRT)、全脑放射治疗(WBRT)或这些治疗方式的组合通常被用于局部治疗。针对 CTLA-4 和 PD-1 免疫检查点受体的抑制性单克隆抗体显著改善了转移性黑色素瘤患者的生存率,包括 MBM 患者。这种延长的生存时间,以及潜在的免疫刺激机制,可能使患者面临更高的长期并发症风险,如脑放射性坏死(RNB)。
我们分析了在一个机构队列中 142 例黑色素瘤患者的发病率,这些患者在接受派姆单抗治疗后进行了前瞻性随访,并在扩展访问计划中接受了治疗。
在 142 例患者中,有 43 例(30.7%)患者在开始使用派姆单抗时患有 MBM。其中,31 例(72.1%)接受 SRS 治疗,8 例(18.6%)接受 WBRT,4 例(9.3%)患者未接受过局部治疗。在接受 RT 的患者中,有 28 例(71.1%)在接受派姆单抗治疗前接受过 RT。有 5 例(12.8%)患者在接受 RT 后 11.15 个月(8-46 个月)中位数时间出现新的症状性假性肿瘤病变。在所有患者中,RNB 的诊断均经放射学证实。2 例患者接受皮质类固醇治疗,2 例患者接受贝伐单抗治疗,3 例症状性患者接受手术治疗。接受手术治疗的患者的诊断得到了组织学证实。
接受 SRS 治疗并对派姆单抗有获益反应的 MBM 黑色素瘤患者存在发生迟发性 RNB 的风险。如果怀疑在先前照射过的 MBM 部位出现孤立性进展,应考虑 RNB 的诊断。