Center for Clinical Documentation and Evaluation (SKDE), Tromsø, Norway.
Department of Community Medicine, UiT-The Arctic University of Norway, Tromsø, Norway.
PLoS One. 2018 Aug 23;13(8):e0202028. doi: 10.1371/journal.pone.0202028. eCollection 2018.
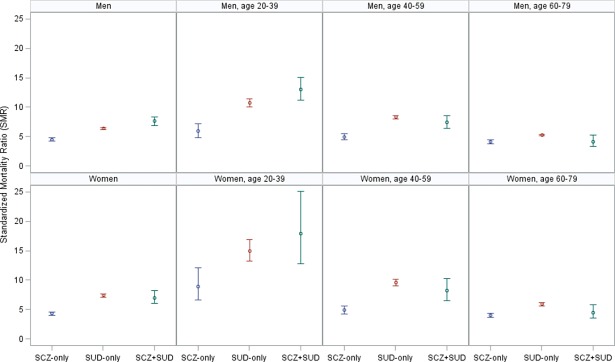
Individuals with schizophrenia or substance use disorder have a substantially increased mortality compared to the general population. Despite a high and probably increasing prevalence of comorbid substance use disorder in people with schizophrenia, the mortality in the comorbid group has been less studied and with contrasting results. We performed a nationwide open cohort study from 2009 to 2015, including all Norwegians aged 20-79 with schizophrenia and/or substance use disorder registered in any specialized health care setting in Norway, a total of 125,744 individuals. There were 12,318 deaths in the cohort, and total, sex-, age- and cause-specific standardized mortality ratios (SMRs) were calculated, comparing the number of deaths in patients with schizophrenia, schizophrenia only, substance use disorder only or a co-occurring diagnosis of schizophrenia and substance use disorder to the number expected if the patients had the age-, sex- and calendar-year specific death rates of the general population. The SMRs were 4.9 (95% CI 4.7-5.1) for all schizophrenia patients, 4.4 (95% CI 4.2-4.6) in patients with schizophrenia without substance use disorder, 6.6 (95% CI 6.5-6.8) in patients with substance use disorder only, and 7.4 (95% CI 7.0-8.2) in patients with both schizophrenia and substance use disorder. The SMRs were elevated in both genders, in all age groups and for all considered causes of death, and most so in the youngest. Approximately 27% of the excess mortality in all patients with schizophrenia was due to the raised mortality in the subgroup with comorbid SUD. The increased mortality in patients with schizophrenia and/or substance use disorder corresponded to more than 10,000 premature deaths, which constituted 84% of all deaths in the cohort. The persistent mortality gap highlights the importance of securing systematic screening and proper access to somatic health care, and a more effective prevention of premature death from external causes in this group.
与普通人群相比,精神分裂症或物质使用障碍患者的死亡率大幅增加。尽管精神分裂症患者合并物质使用障碍的患病率很高,且可能呈上升趋势,但对合并组的死亡率研究较少,且结果存在差异。我们进行了一项全国性的开放队列研究,纳入了 2009 年至 2015 年期间所有在挪威任何专门医疗保健机构登记的年龄在 20-79 岁的患有精神分裂症和/或物质使用障碍的挪威人,共 125744 人。该队列中有 12318 人死亡,计算了总死亡率、性别特异性死亡率、年龄特异性死亡率和死因特异性标准化死亡率比(SMR),将精神分裂症患者、仅有精神分裂症、仅有物质使用障碍或同时患有精神分裂症和物质使用障碍患者的死亡人数与如果患者具有普通人群的年龄、性别和日历特定死亡率,则预期的死亡人数进行比较。所有精神分裂症患者的 SMR 为 4.9(95%CI 4.7-5.1),无物质使用障碍的精神分裂症患者的 SMR 为 4.4(95%CI 4.2-4.6),仅有物质使用障碍的患者的 SMR 为 6.6(95%CI 6.5-6.8),同时患有精神分裂症和物质使用障碍的患者的 SMR 为 7.4(95%CI 7.0-8.2)。在所有性别、所有年龄组和所有考虑的死因中,SMR 均升高,在最年轻的人群中升高最为明显。大约 27%的所有精神分裂症患者的超额死亡率归因于合并 SUD 亚组的死亡率升高。精神分裂症和/或物质使用障碍患者的死亡率升高导致超过 10000 人过早死亡,占队列总死亡人数的 84%。持续存在的死亡率差距凸显了确保系统筛查和获得适当的躯体保健的重要性,以及更有效地预防该人群的意外伤害性死亡。