Lobo Niyati, Thurairaja Ramesh, Nair Rajesh, Dasgupta Prokar, Khan Muhammad Shamim
Department of Urology, Brighton and Sussex University Hospitals NHS Trust, Brighton, UK.
Department of Urology, Guy's Hospital, London, UK.
Arab J Urol. 2018 Apr 11;16(3):307-313. doi: 10.1016/j.aju.2018.01.006. eCollection 2018 Sep.
To investigate whether a totally intracorporeally radical cystectomy (RC) can be considered the new 'gold standard' in bladder cancer, as open RC (ORC) is the current 'gold standard' for surgical treatment of muscle-invasive and high-grade non-muscle-invasive bladder cancer. However, robot-assisted radical cystectomy (RARC) is becoming the preferred surgical approach in many centres as it seems to maintain the oncological control of open surgery whilst offering improved perioperative benefits.
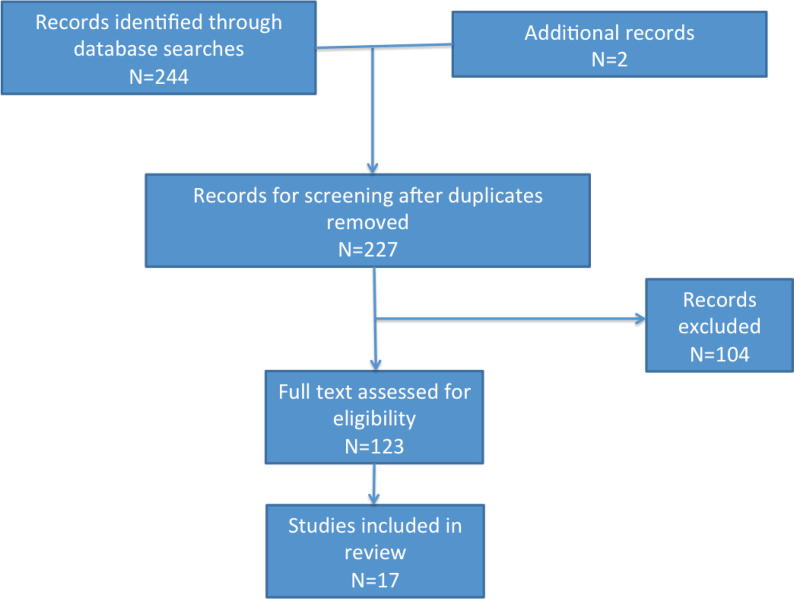
A review of the literature was conducted using the Pubmed/MEDLINE, ISI Web of Knowledge and Cochrane Databases to identify studies that included both ORC and RARC with intracorporeal and extracorporeal urinary diversion (UD) published up to July 2017.
Evidence from four single-centre randomised controlled trials and now the multicentre Randomized Trial of Open versus Robotic Cystectomy (RAZOR) trial demonstrate the oncological equivalence of RARC to ORC. The only convincing evidence for the superiority of RARC is in the area of blood loss and transfusion rates. However, the UD procedure in these trials was performed extracorporeally and, to realise the full benefits of RARC, a totally intracorporeal approach is needed. Intracorporeal UDs (ICUDs) have been shown to be technically feasible by a few expert centres and have demonstrated some improved short-term perioperative outcomes compared to extracorporeal UDs.
Although initial outcomes appear promising, RARC with ICUD is far from gaining 'gold standard' status. Further studies are needed to confirm that outcomes are reproducible widely. Furthermore, the benefits of a totally intracorporeal approach must be confirmed in randomised controlled trials.
探讨完全腹腔镜下根治性膀胱切除术(RC)是否可被视为膀胱癌治疗的新“金标准”,因为开放根治性膀胱切除术(ORC)是目前治疗肌层浸润性和高级别非肌层浸润性膀胱癌的“金标准”。然而,机器人辅助根治性膀胱切除术(RARC)在许多中心正成为首选的手术方式,因为它似乎能维持开放手术的肿瘤学控制效果,同时在围手术期带来更多益处。
通过Pubmed/MEDLINE、ISI Web of Knowledge和Cochrane数据库对文献进行综述,以确定截至2017年7月发表的包含ORC和RARC以及体内和体外尿流改道(UD)的研究。
四项单中心随机对照试验以及现在的多中心开放与机器人膀胱切除术随机试验(RAZOR)的证据表明,RARC与ORC在肿瘤学效果上相当。RARC优越性的唯一令人信服的证据在于失血和输血率方面。然而,这些试验中的尿流改道手术是在体外进行的,为了充分实现RARC的益处,需要采用完全腹腔镜入路。一些专家中心已证明体内尿流改道(ICUD)在技术上是可行的,并且与体外尿流改道相比,已显示出一些改善的短期围手术期结果。
尽管初步结果看起来很有前景,但采用ICUD的RARC远未获得“金标准”地位。需要进一步研究以确认结果具有广泛的可重复性。此外,完全腹腔镜入路的益处必须在随机对照试验中得到证实。