Department of Pulmonary Medicine, Shanghai Chest Hospital, Shanghai Jiaotong University, Shanghai, China.
Department of Thoracic Sugery, Shanghai Chest Hospital, Shanghai Jiaotong University, Shanghai, China.
Oncologist. 2019 Feb;24(2):157-e64. doi: 10.1634/theoncologist.2018-0120. Epub 2018 Aug 29.
The findings of this prospective, single-arm, phase II study showed that neoadjuvant erlotinib was well tolerated and might improve the radical resection rate in patients with stage IIIA-N2 epidermal growth factor receptor mutation-positive non-small cell lung cancer (NSCLC).Erlotinib shows promise as a neoadjuvant therapy option in this patient population.Next-generation sequencing may be useful for predicting outcomes with preoperative tyrosine kinase inhibitors (TKIs) in patients with NSCLC.Large-scale randomized controlled trials investigating the role of TKIs in perioperative therapy, combining neoadjuvant and adjuvant treatments to enhance personalized therapy for patients in this precision medicine era, are warranted.
Information on epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) as neoadjuvant therapy in non-small cell lung cancer (NSCLC) is scarce. We evaluated whether neoadjuvant erlotinib improves operability and survival in patients with stage IIIA-N2 mutation-positive NSCLC.
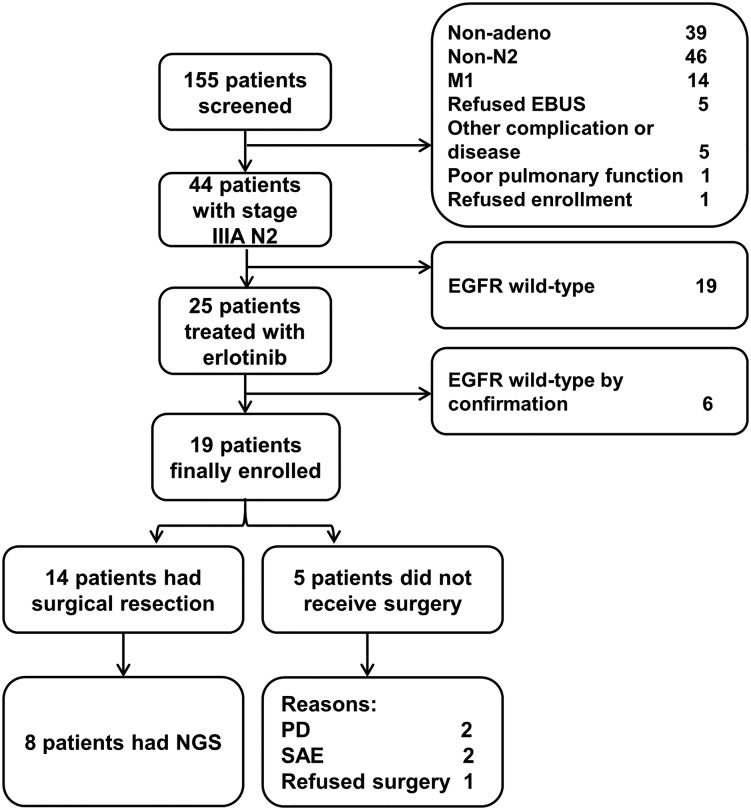
We conducted a prospective, single-arm, phase II study. Patients received erlotinib 150 mg per day for 56 days in the neoadjuvant period. The primary endpoint was the radical resection rate.
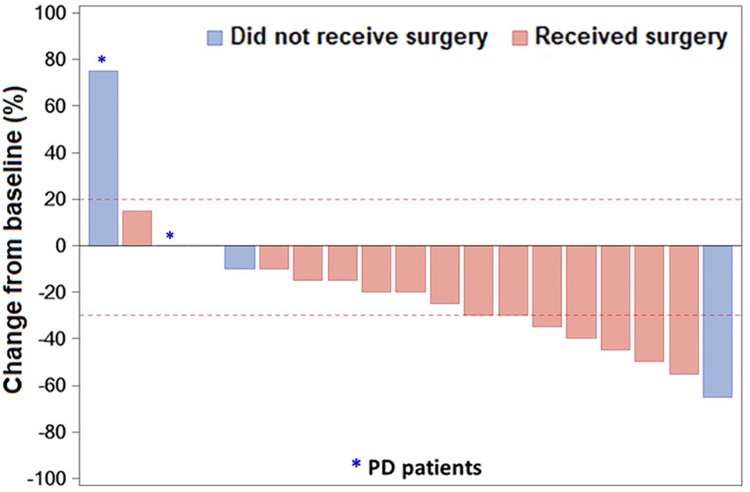
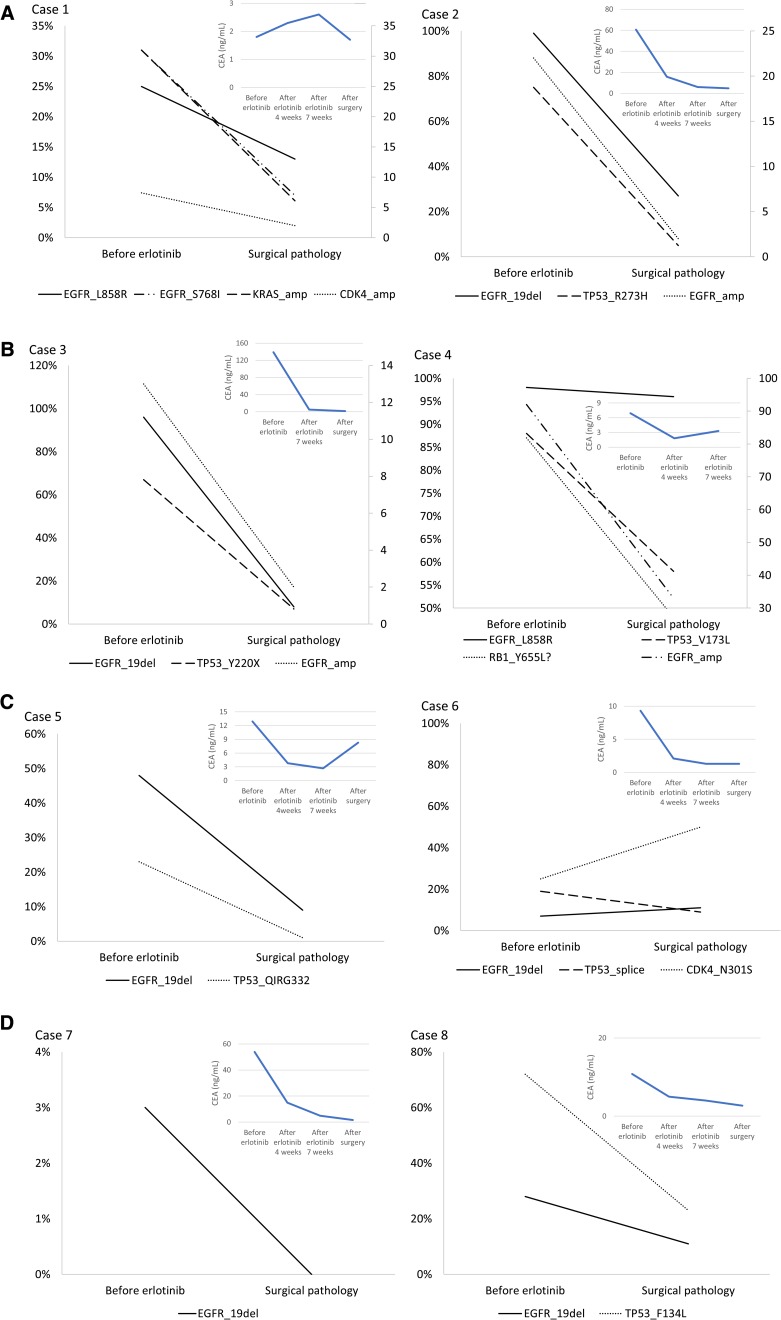
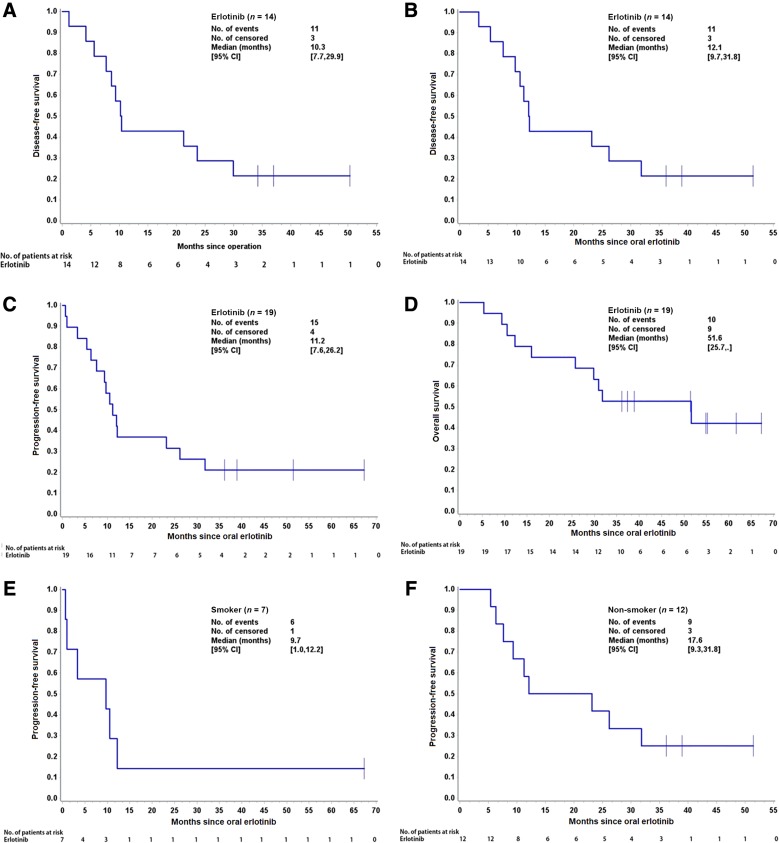
Nineteen patients were included in the final analysis. After erlotinib treatment, 14 patients underwent surgery. The radical resection rate was 68.4% (13/19) with a 21.1% (4/19) rate of pathological downstaging. The objective response rate was 42.1%; 89.5% (17/19) of patients achieved disease control, with a 10.3-month median disease-free survival among patients who underwent surgery. Among all 19 patients who received neoadjuvant therapy, median progression-free survival (PFS) and overall survival were 11.2 and 51.6 months, respectively. Adverse events (AEs) occurred in 36.8% (7/19) of patients, with the most common AE being rash (26.3%); 15.8% experienced grade 3/4 AEs. Quality of life (QoL) improvements were observed after treatment with erlotinib for almost all QoL assessments. Effects of mutation on prognosis were evaluated in eight patients with adequate tissue samples. Next-generation sequencing revealed that most patients had a gene mutation (7/8) in addition to an mutation. No mutation, or very low abundance, was associated with longer PFS (36 and 38 months, respectively), whereas high abundance was associated with short PFS (8 months).
Neoadjuvant erlotinib was well tolerated and may improve the radical resection rate in this patient population. Next-generation sequencing may predict outcomes with preoperative TKIs.
这项前瞻性、单臂、二期研究的结果表明,新辅助厄洛替尼耐受良好,并可能提高 IIIA-N2 期表皮生长因子受体突变阳性非小细胞肺癌(NSCLC)患者的根治性切除率。厄洛替尼有望成为此类患者的新辅助治疗选择。下一代测序可能有助于预测 NSCLC 患者术前酪氨酸激酶抑制剂(TKI)的疗效。需要开展大规模的随机对照试验,研究 TKI 在围手术期治疗中的作用,结合新辅助和辅助治疗,以增强精准医学时代此类患者的个体化治疗。
关于表皮生长因子受体(EGFR)酪氨酸激酶抑制剂(TKI)作为 NSCLC 新辅助治疗的信息有限。我们评估了新辅助厄洛替尼是否能提高 IIIA-N2 期 EGFR 突变阳性 NSCLC 患者的手术可行性和生存率。
我们开展了一项前瞻性、单臂、二期研究。患者在新辅助期每天接受厄洛替尼 150mg,共 56 天。主要终点是根治性切除率。
19 例患者最终纳入分析。接受厄洛替尼治疗后,14 例患者接受了手术。根治性切除率为 68.4%(13/19),病理降期率为 21.1%(4/19)。客观缓解率为 42.1%;89.5%(17/19)的患者疾病得到控制,手术患者的中位无疾病生存期为 10.3 个月。在所有接受新辅助治疗的 19 例患者中,中位无进展生存期(PFS)和总生存期分别为 11.2 个月和 51.6 个月。36.8%(7/19)的患者发生不良反应(AE),最常见的 AE 为皮疹(26.3%);15.8%的患者发生 3/4 级 AE。接受厄洛替尼治疗后,几乎所有的生活质量(QoL)评估均观察到 QoL 改善。在 8 例有足够组织样本的患者中评估了 突变对预后的影响。下一代测序显示,除了 突变外,大多数患者都有 基因突变(7/8)。 突变或非常低丰度与较长的 PFS 相关(分别为 36 和 38 个月),而高丰度与较短的 PFS 相关(8 个月)。
新辅助厄洛替尼耐受良好,并可能提高此类患者人群的根治性切除率。下一代测序可能有助于预测术前 TKI 的疗效。